Aesthetic Occipital Surgery for Back of Head Reshaping
On this Page
Flat Back of the Head
One of the most common aesthetic deformities of the entire skull is the flat back of the head. Well known to occur from sleeping positions in infants and predisposed to occur in certain ethnic groups, lack of a nice shape to the back of the head can be aesthetically disturbing. It occurs in a wide variety of presentations that differ in location (mid-occipital and crown flatness), plagiocephalic (one-sided) vs brachycephalic (both sides) and extent of missing occipital projection.
While the occurrence of these occipital shape disturbances occur in both women and men, there are some unique gender differences. Women tend to be highly focused on the lack of projection in the crown area which is really the junction of the top of the back of the head whose upper extent goes onto the top of the skull. A male’s concern is often lack of mid-occipital projection or asymmetry of the two sides of the back of the head. Both types of gender occipital deformities often involve elaborate and time consuming methods of hair camouflage on the part of the patient.
Occipital augmentation can be done using intraoperatively applied bone cements (usually PMMA) or with the fabrication of custom implants. While long scalp incisions make the use of either augmentation material much easier, they are understandably not aesthetically acceptable for most patients. The use of smaller incisions and the unique requirements of intraoperative positioning can make occipital augmentation surgery challenging.
PMMA can be applied through incision lengths of 5cm to 8cms depending on the size of the defect and the volume of material needed. This requires external manipulation and shaping of the material as it sets with great attention paid to creating smooth edge transitions. The incision can be placed high near the crown or low at the bottom of the hairline depending upon the location of the occipital augmentation needed and the patient’s hair density and pattern.




Preoperative shaping of an occipital implant through a custom 3D design process makes any larger occipital deficiency more assured with a lower risk of potential revision. Even a large custom occipital implant, because it is made of solid silicone and has some flexibility, permits it to be inserted through a much smaller incision than one would envision possible.







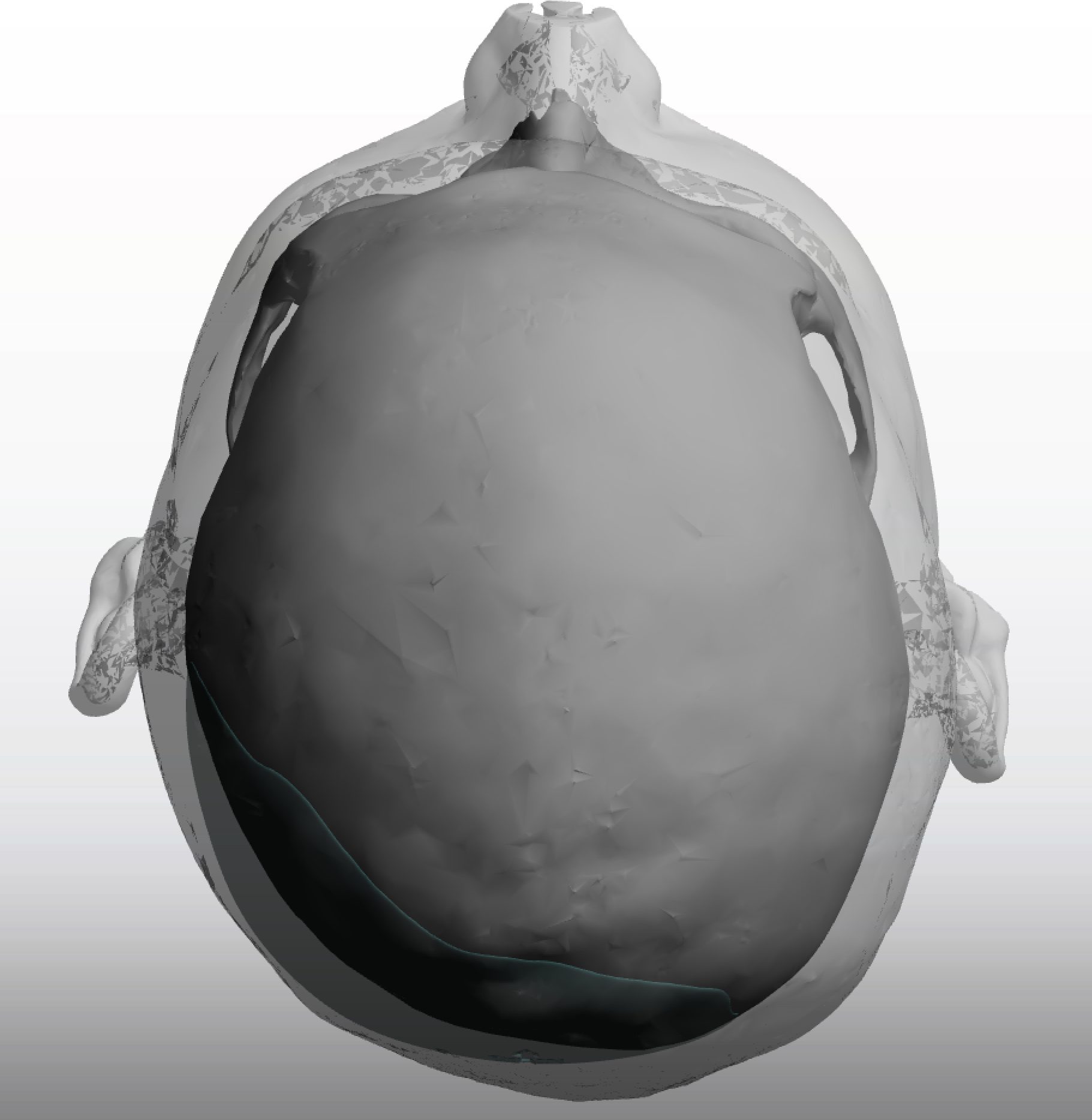

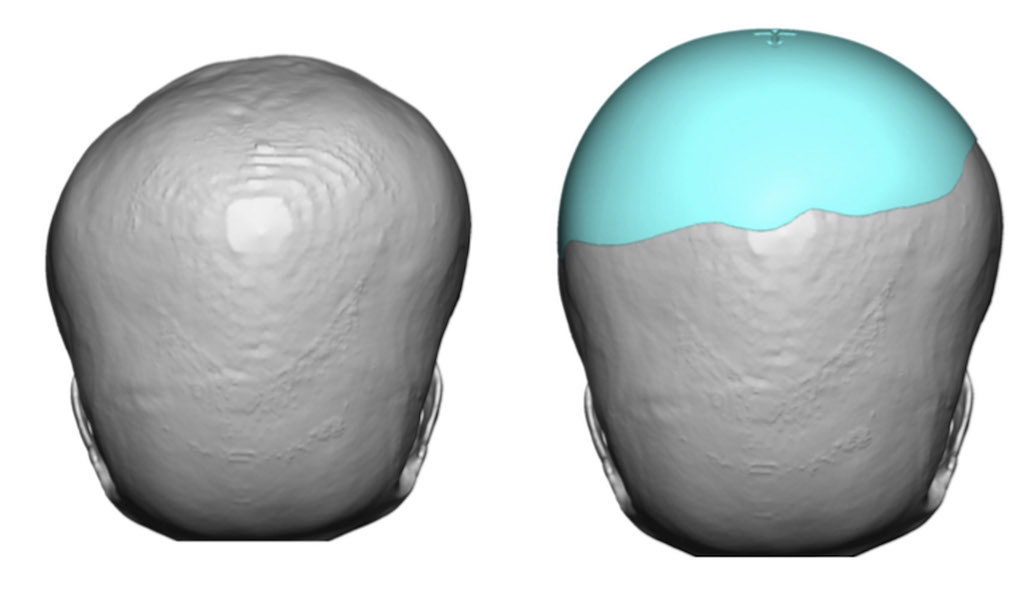
There are many variations of back of the head skull deformities of which plagiocephaly is the most known. Flattening of the upper part of the back of the head or the crown area usually comes from a flattening or lack of adequate bone thickness over the original posterior fontanelle area seen in babies. A custom skull implant can be used to build that area up and have it blend into the surrounding skull areas.



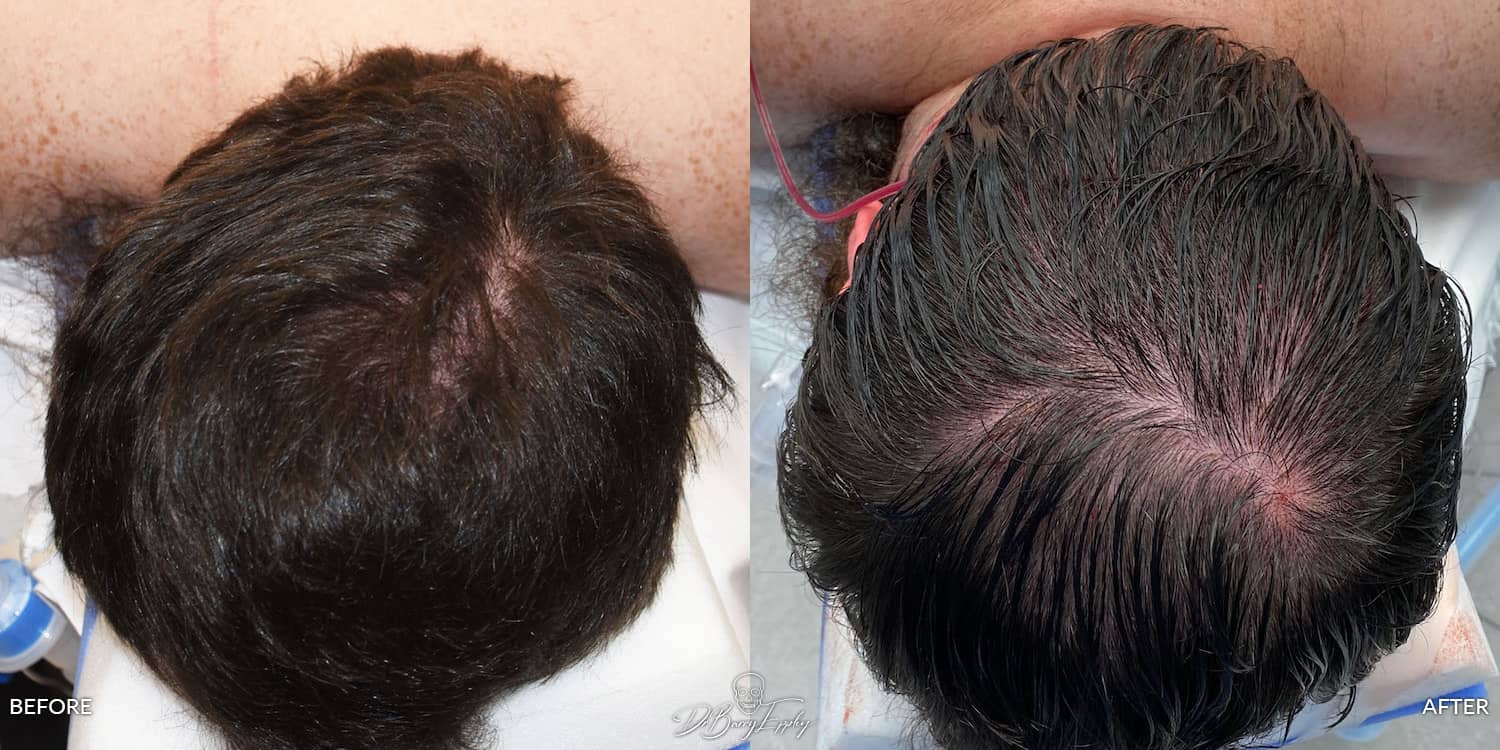
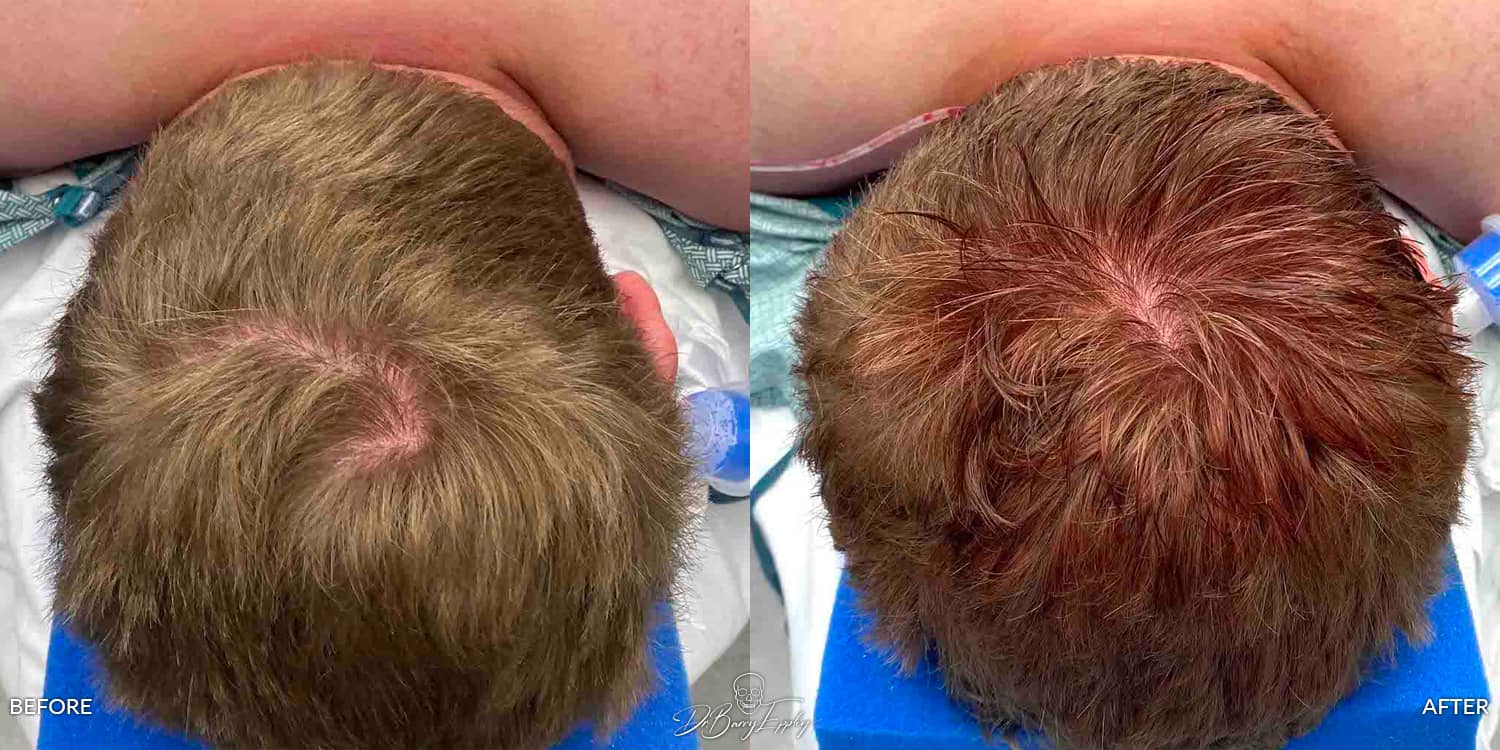
It also not uncommon that if there are other areas of the head shape/skull that needs to be addressed along with a flat back of the head these can all be done during the same surgery. Many of these surrounding problems are often the result of the plagiocephaly even if they are of less magnitude than the flat back of the head. Here is a case example of the simultaneous need for a large back of the head augmentation, posterior sagittal ridge reduction and right temporal reduction as a result of congenital plagiocephaly…all done through only one visible small incision on the top of the head. (the one behind the ear is invisible)

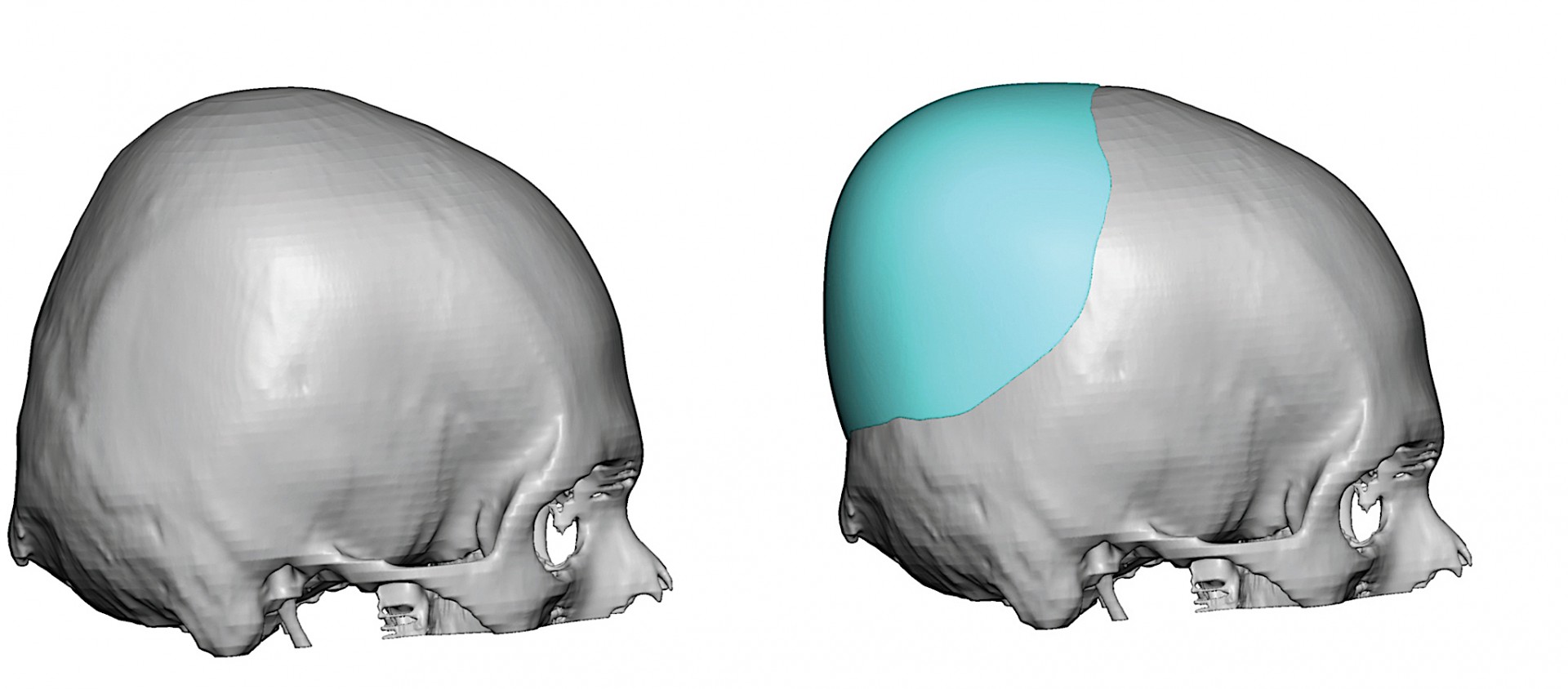
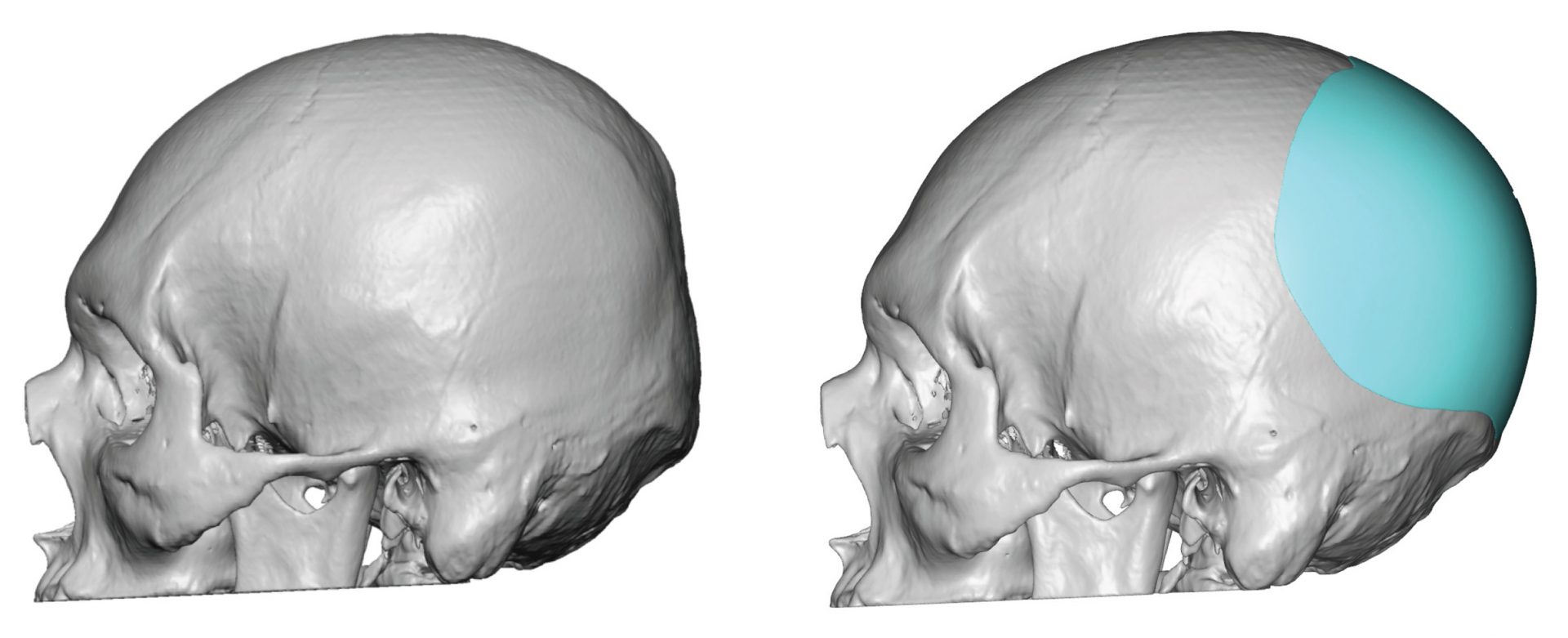
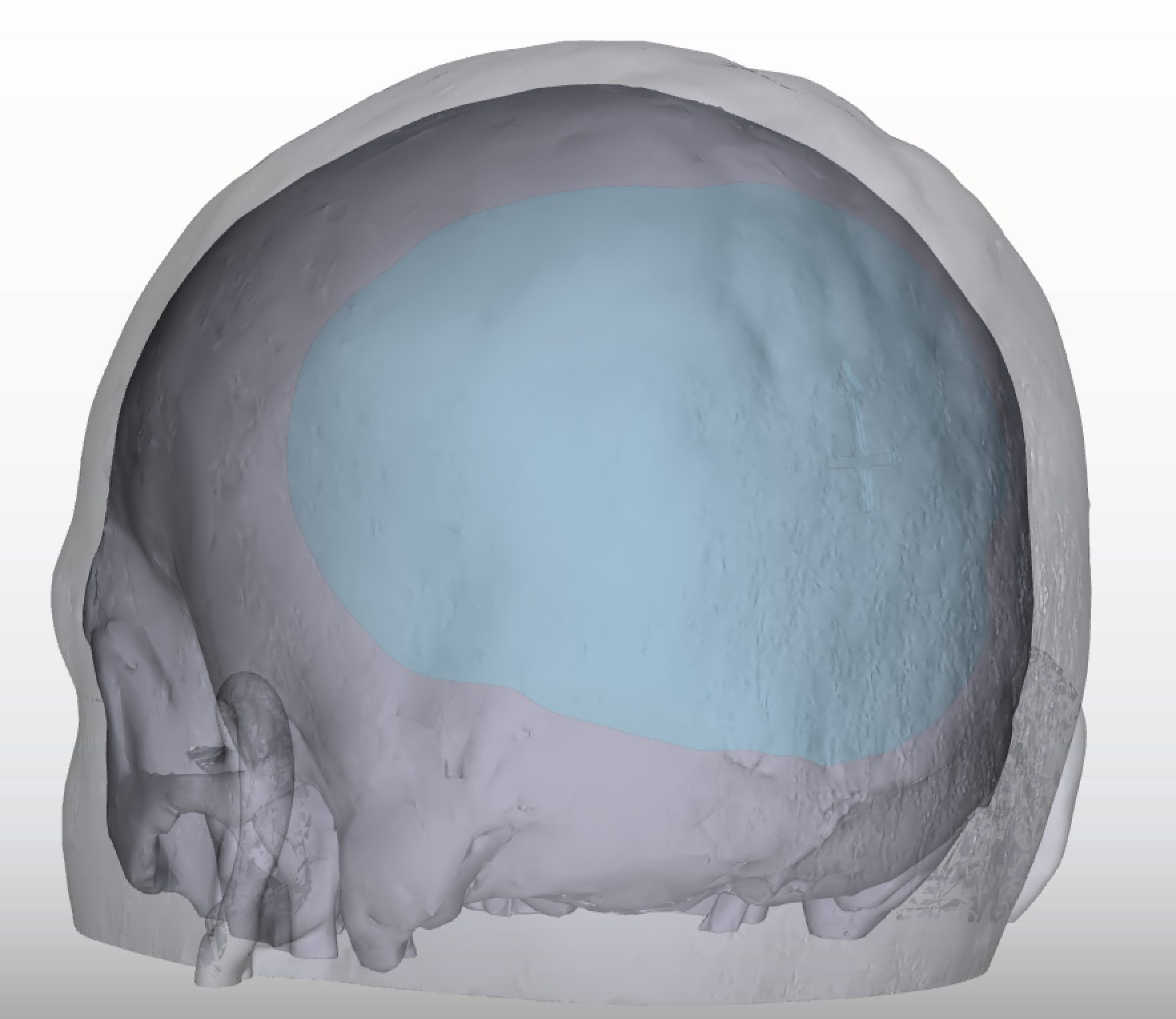
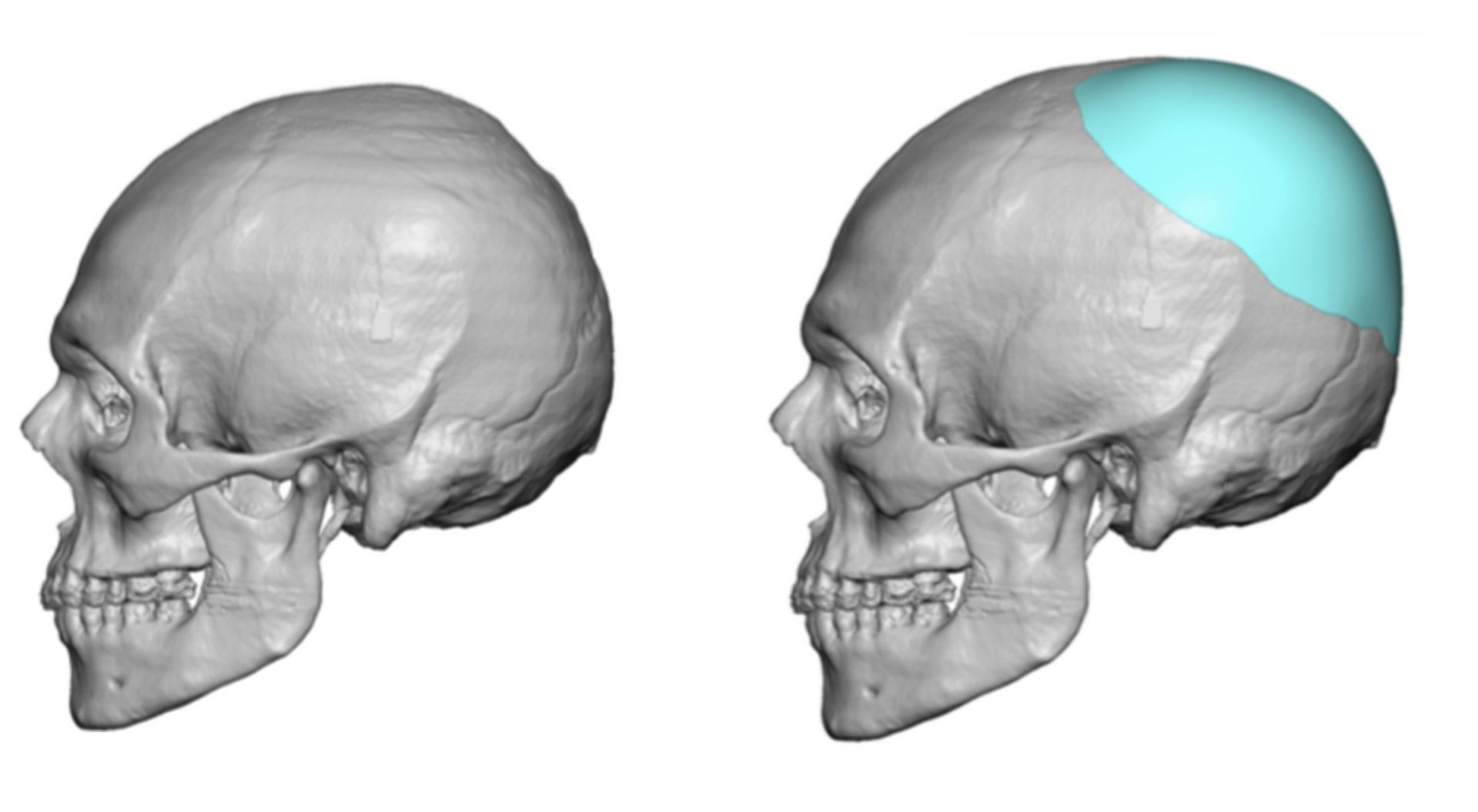
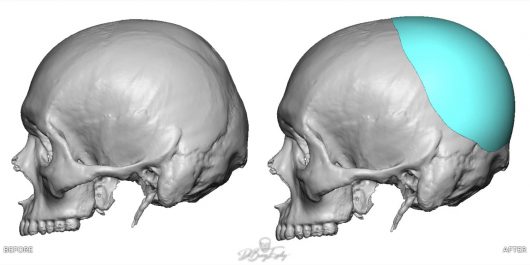
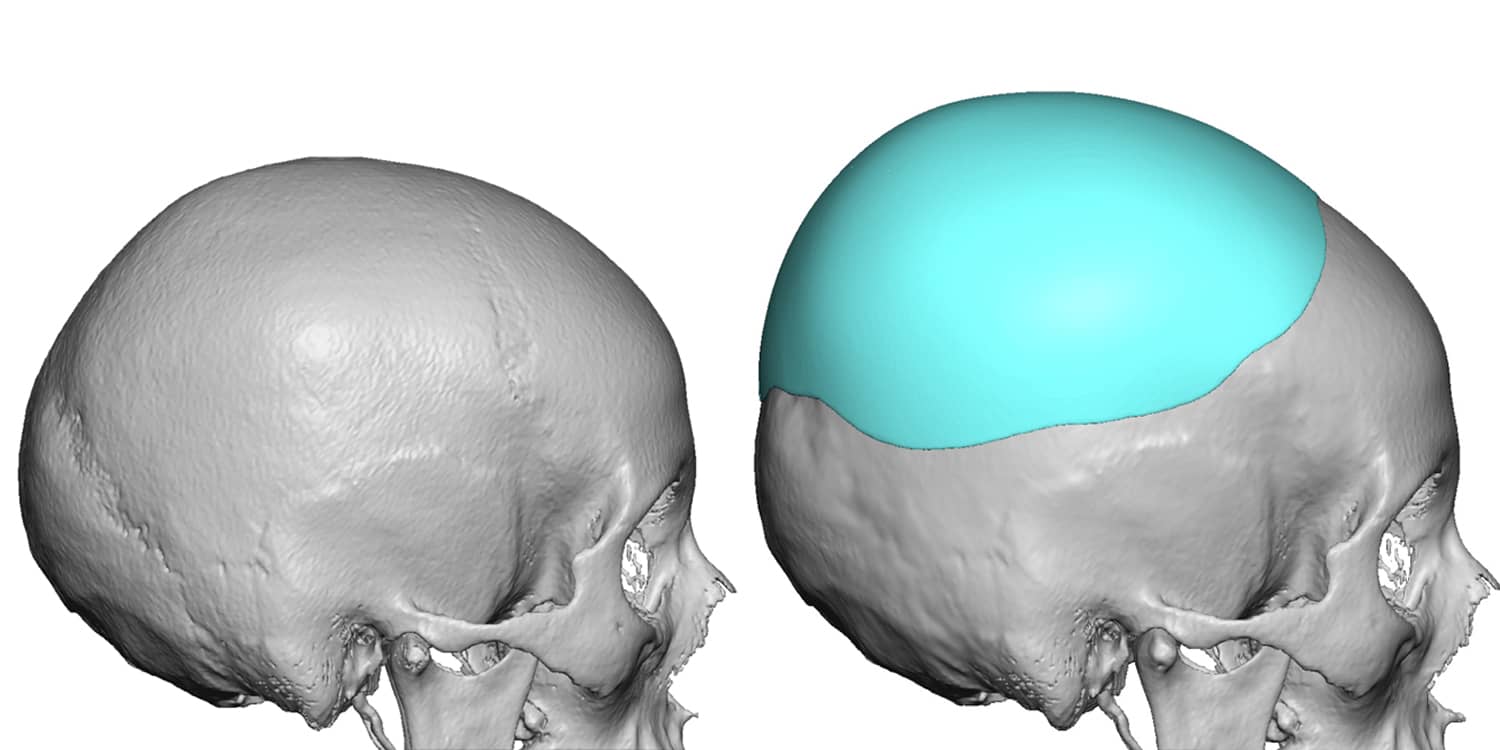
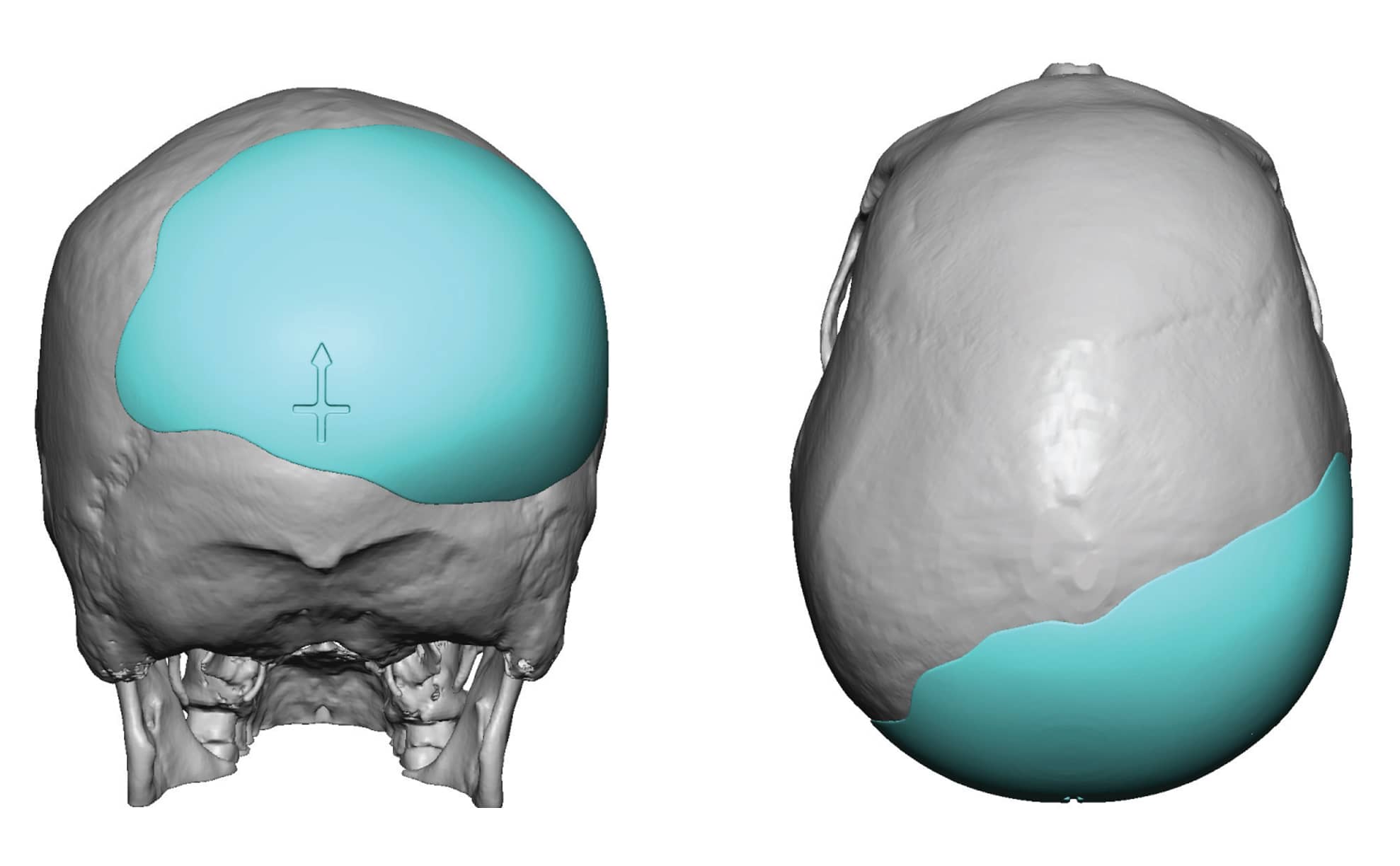
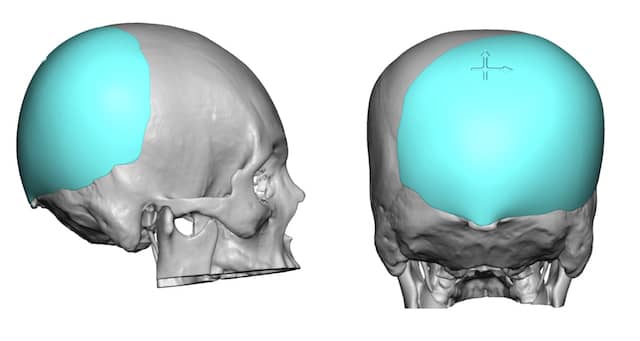
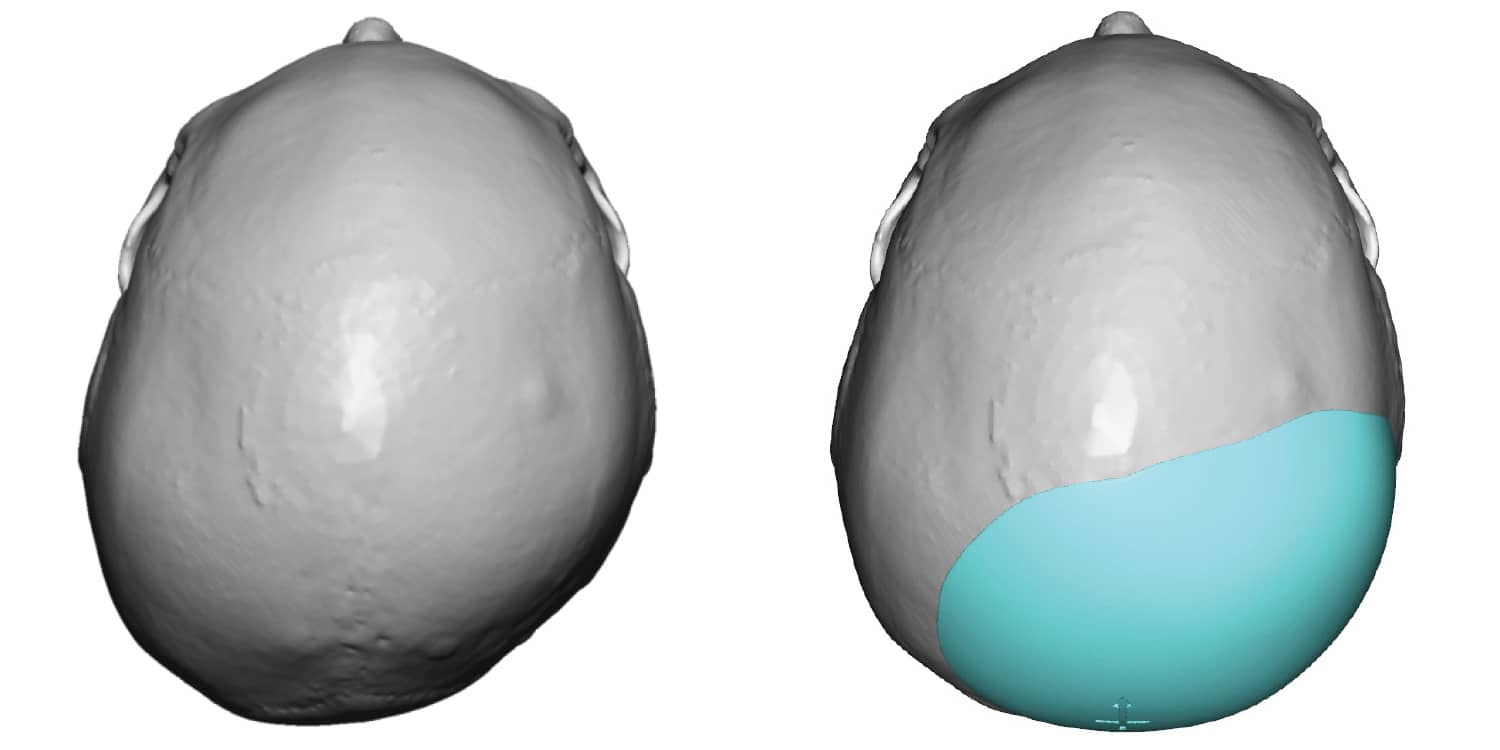
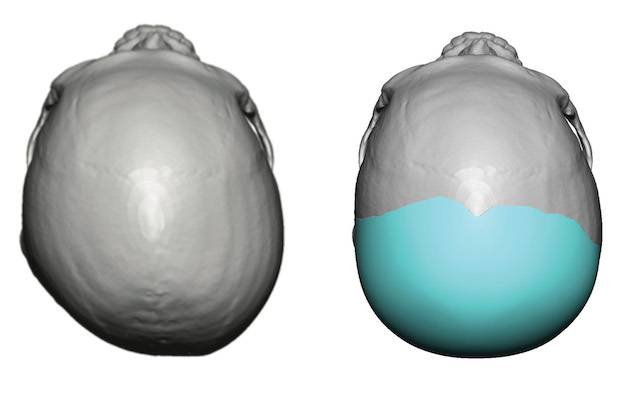
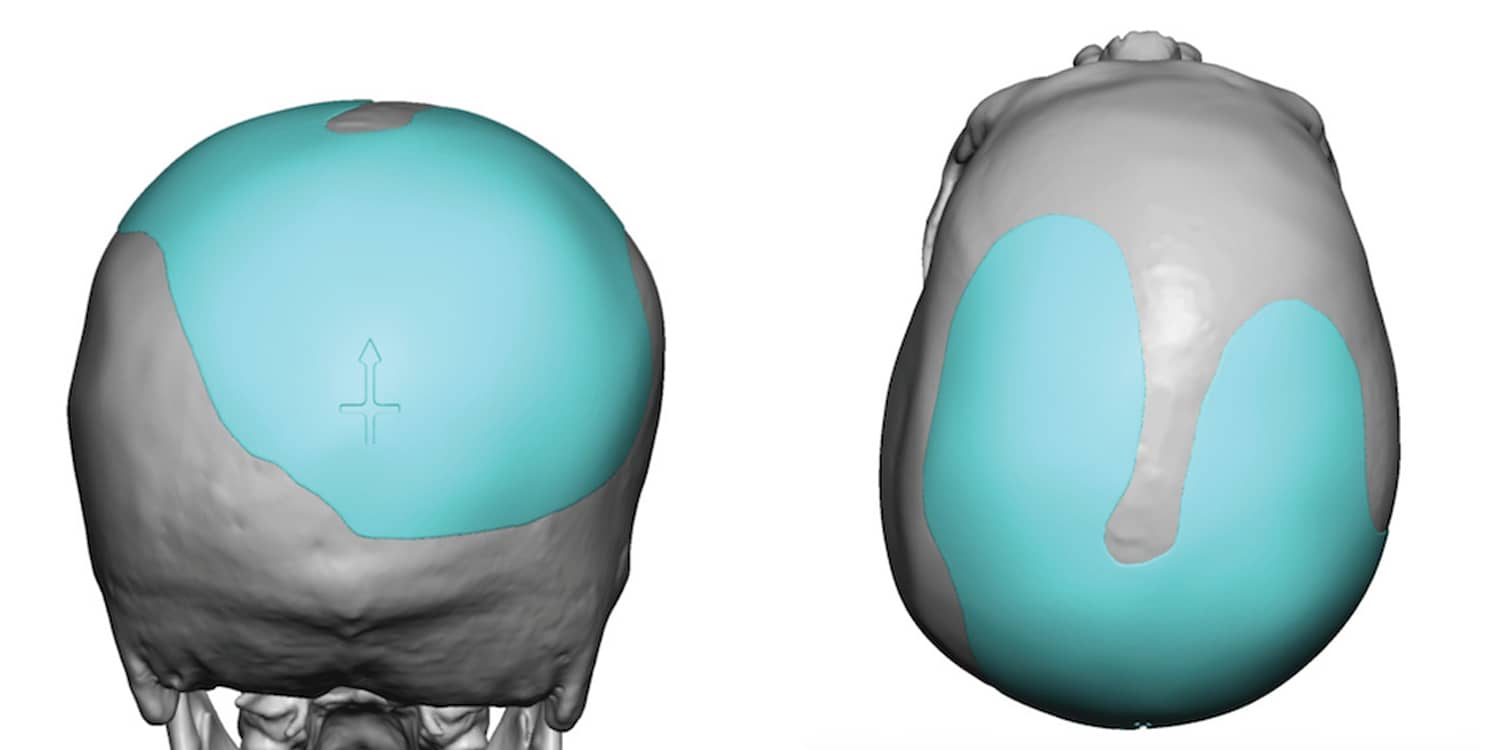
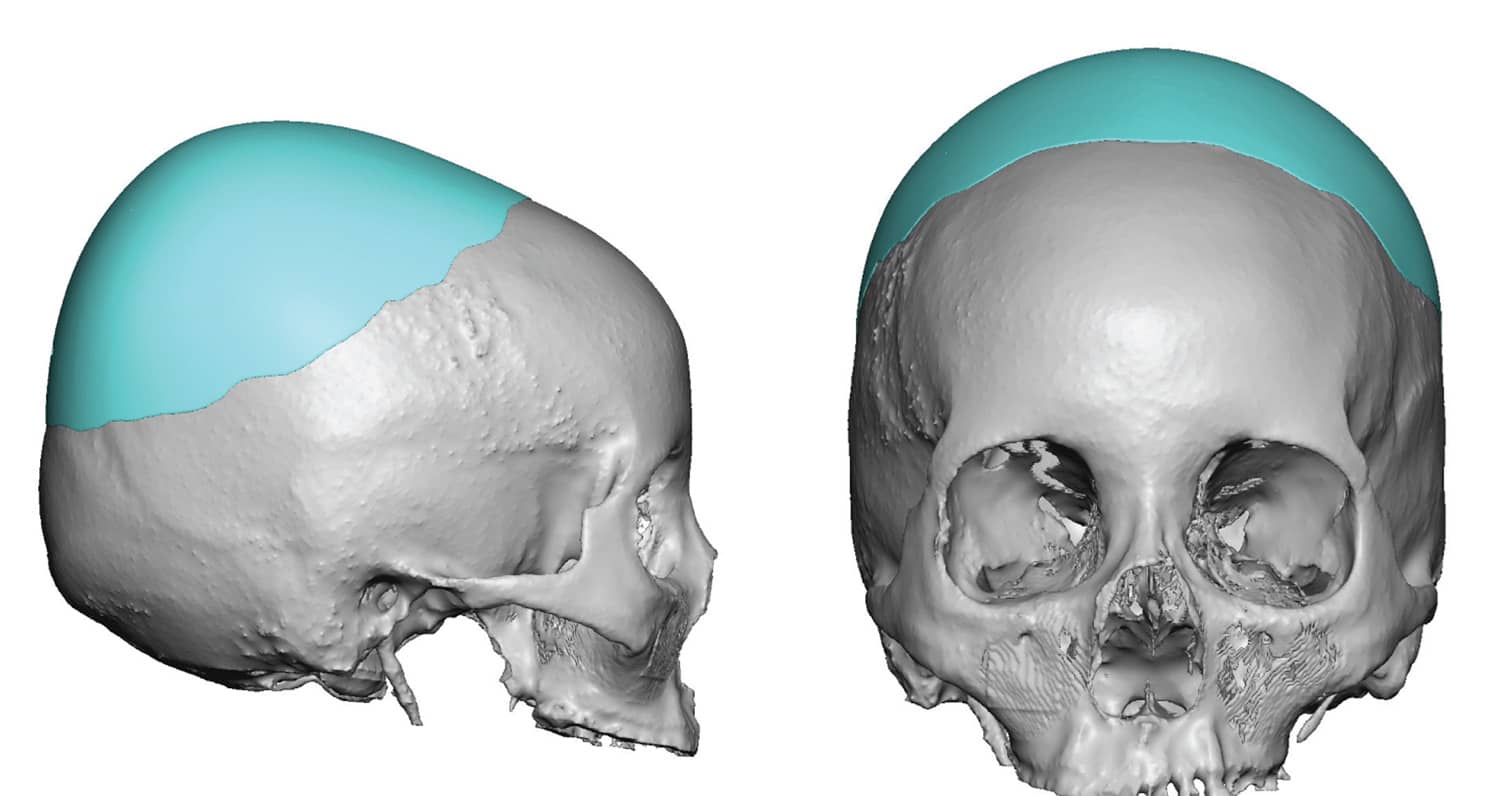
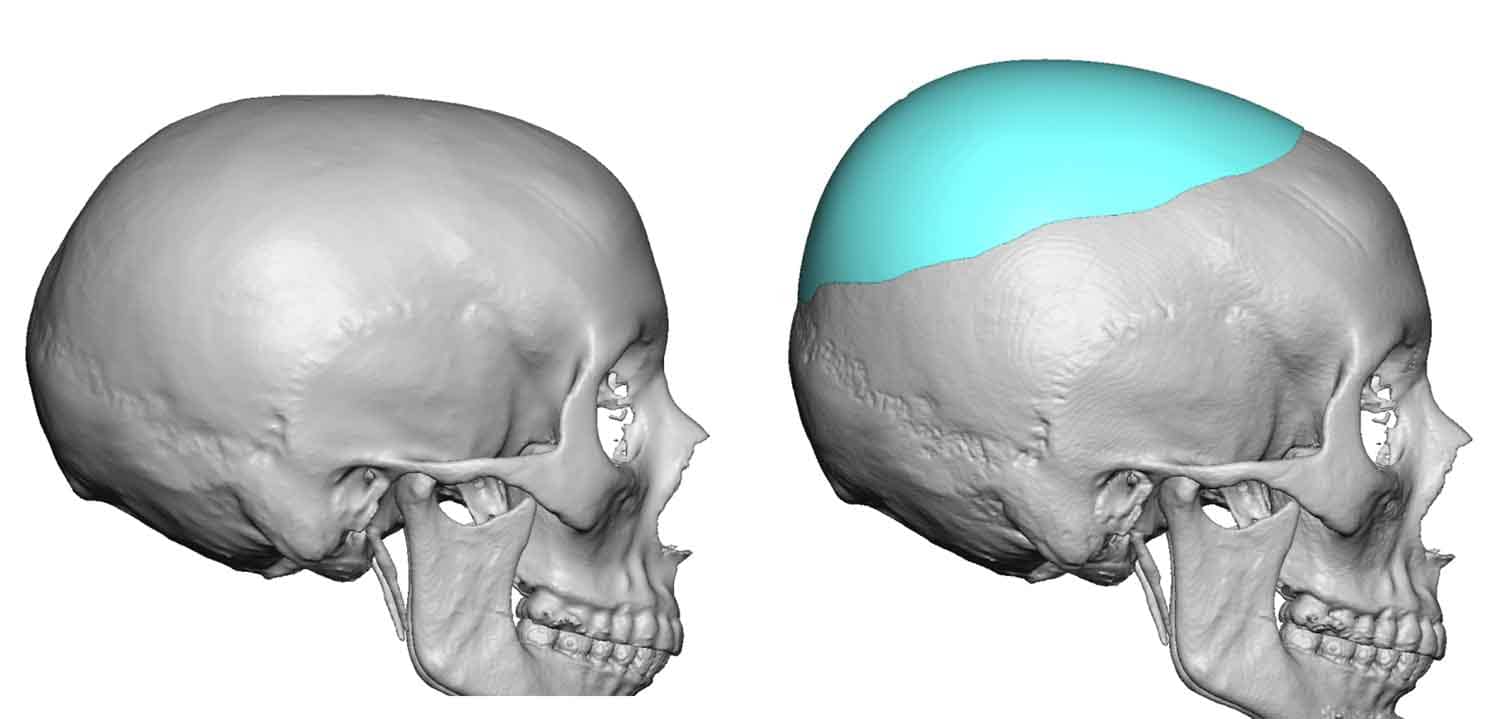
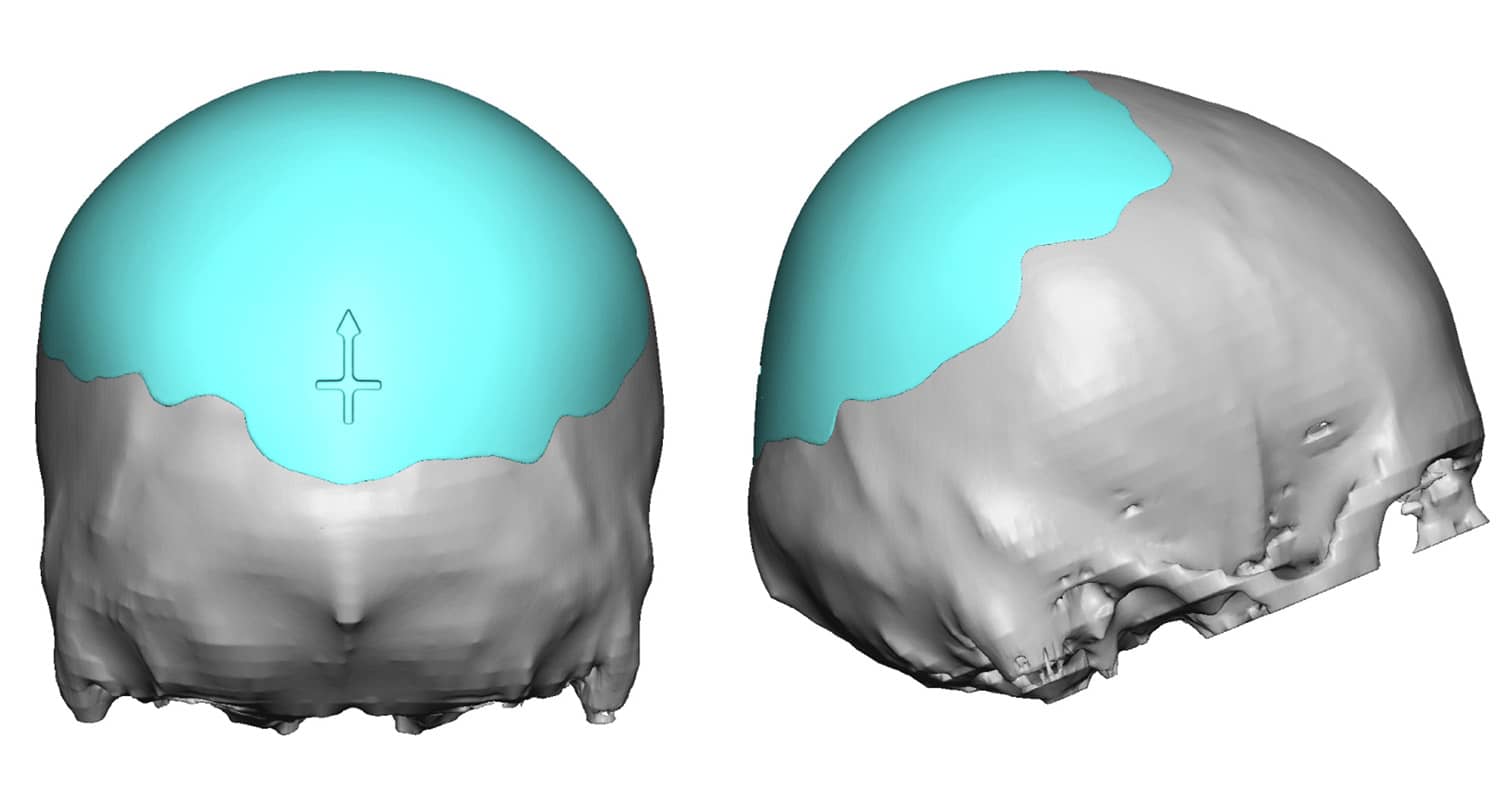
While plagiocephaly is the most common aesthetic back of the head deficiency, both sides of the back of the head may be equally flat. From a craniofacial perspective this is known as brachycephaly. In essence the entire back of the head to have more projection. In these cases the custom skull implant covers the entire back of the head (technically the occipital-parieta regions) as well as blends into the posterior temporal regions for a smooth and blended shape.


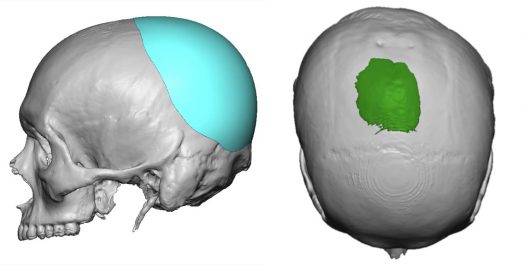
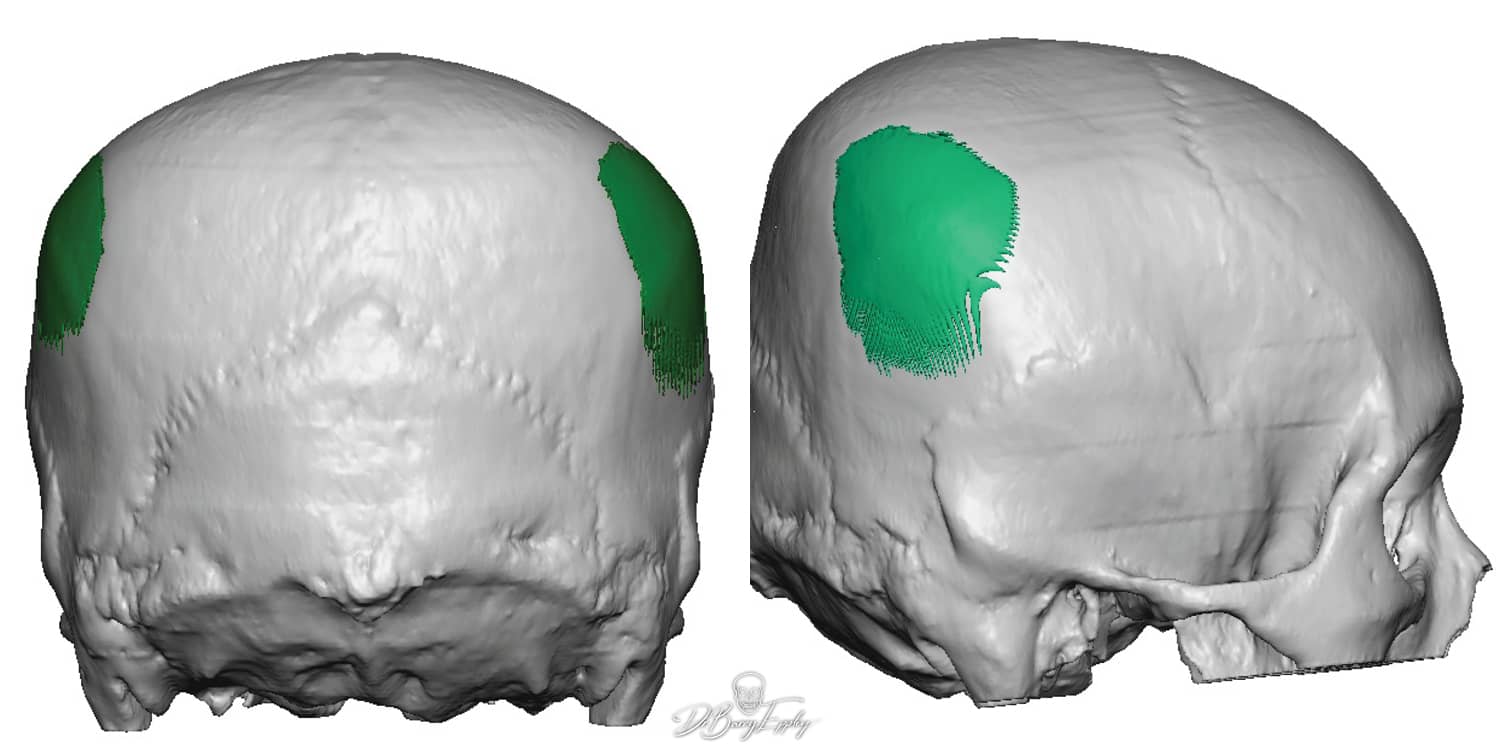
In some cases of brachycephaly or flattening of the entire back of the head reduction of the widened parietal-temporal regions may need to be done. This requires small vertical incisions directly over the widened ‘points’ at the parietal-temporal areas for removal of some of the posterior temporal muscle as well as burring down some of the bone. Such skull area reductions are often done in combination with a custom skull implant to improve the projection on the back of the head.

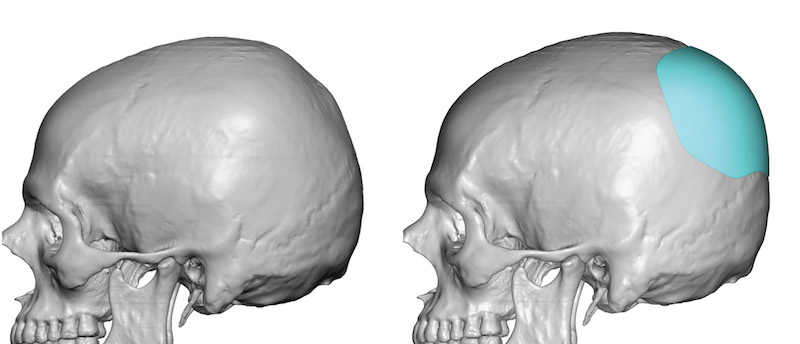
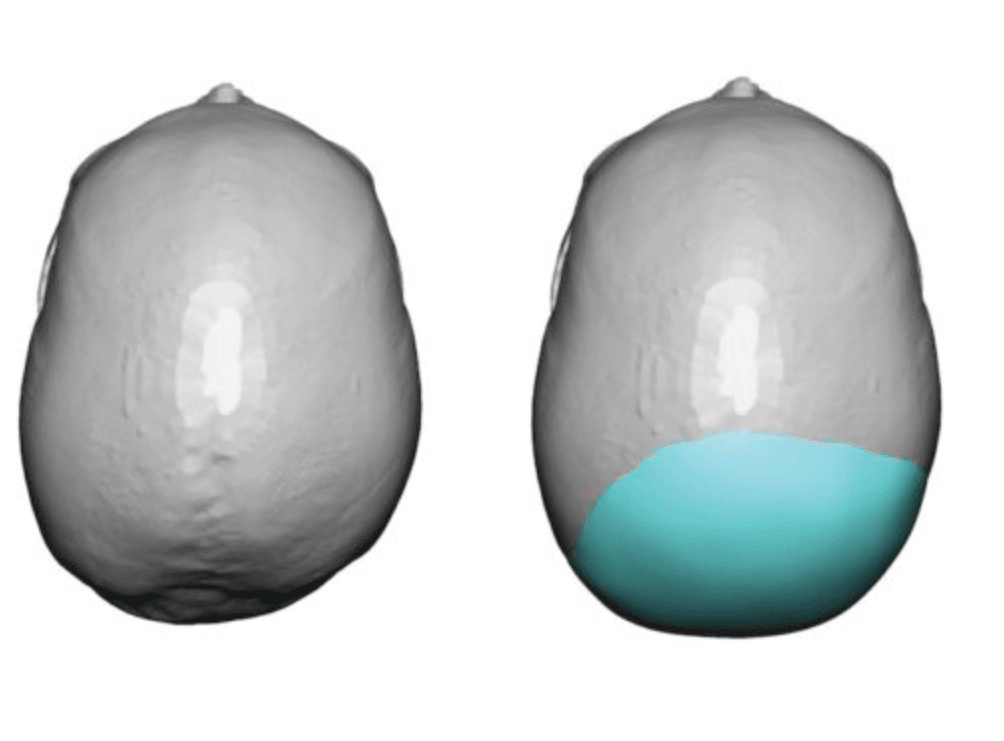
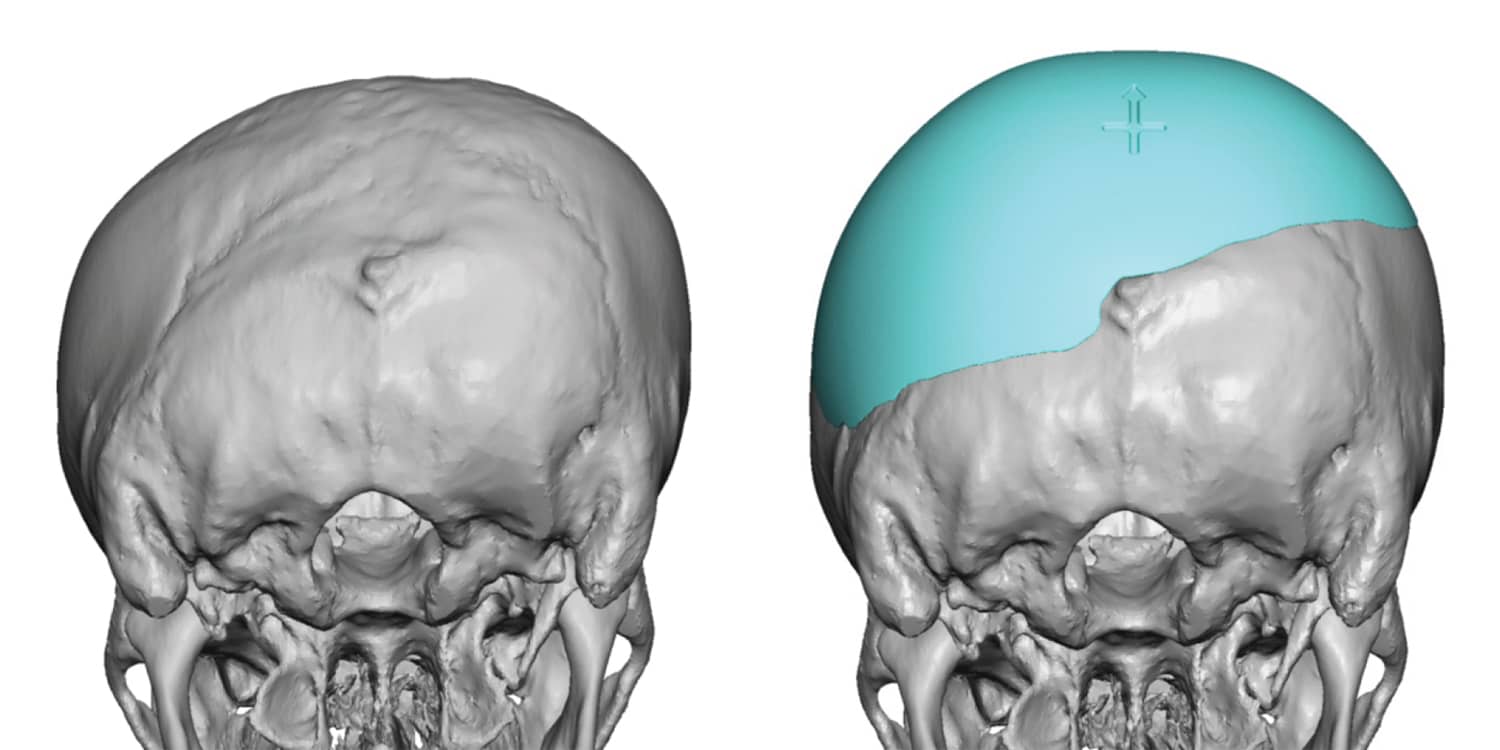
Another unique back of the head flattening of the skull that can occur is what I call the posterior fontanelle deformity. The crown of the skull is the adult shape of the original posterior fontanelle or soft spot in a baby. How well the cranial bones close this temporary skull defect and how effectively it ossifies determines both the thickness and shape of this curved area of the skull. In some people the crown areas is flatter as a result of an ‘incompletion’ of this process. This lack of crown projection in an adult can be effectively corrected with a custom skull implant design.
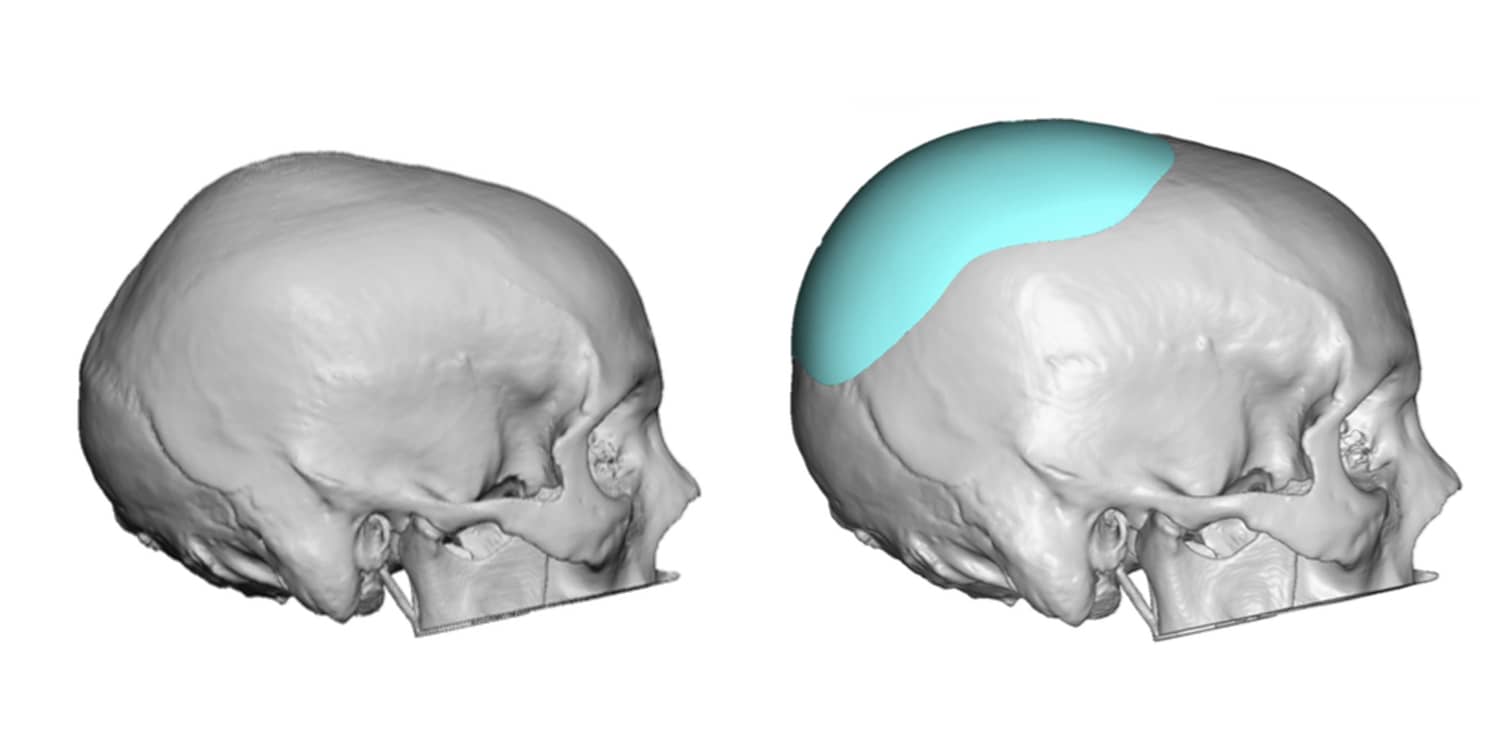


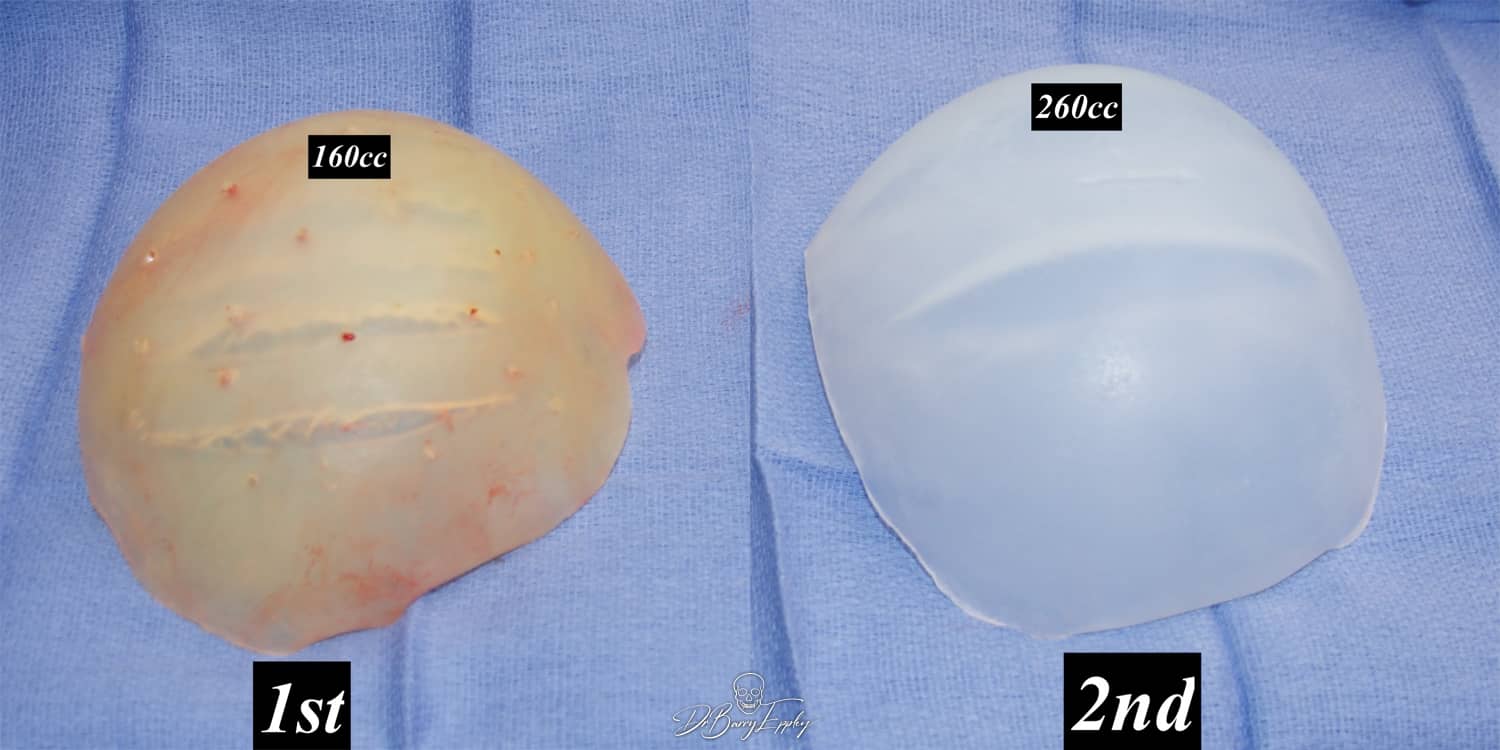
While a custom implant is the ideal approach for back of the head augmentation, when doing a larger head augmentation, you must factor in how much the scalp can stretch to accommodate it. Some congenitally flat back of the heads also have a scalp ‘deficiency’ when the bone surface is expanded. Based on how much back of the head augmentation a patient desires a two-stage approach may be needed to allow a larger implant to be placed. In the first stage a scalp tissue expander is placed followed six weeks later by the placement of the occipital scalp implant.

The alternative to an up front two stage back of head skull augmentation is what I can an unintentional delayed two stage approach. This is when when the patient feels that whatever implant volume the scalp can stretch to accommodate it initially will be adequate. While that its effective for many patients, some come back years later and desire a new larger custom implant for the back of the head. Since the initial skull implant does have a scalp expansion effect, a larger implant volume is possible. As a general guideline a 50% to 66% volume increase over the first implant is always possible.

Back of Head Contour Asymmetry (Plagiocephaly)
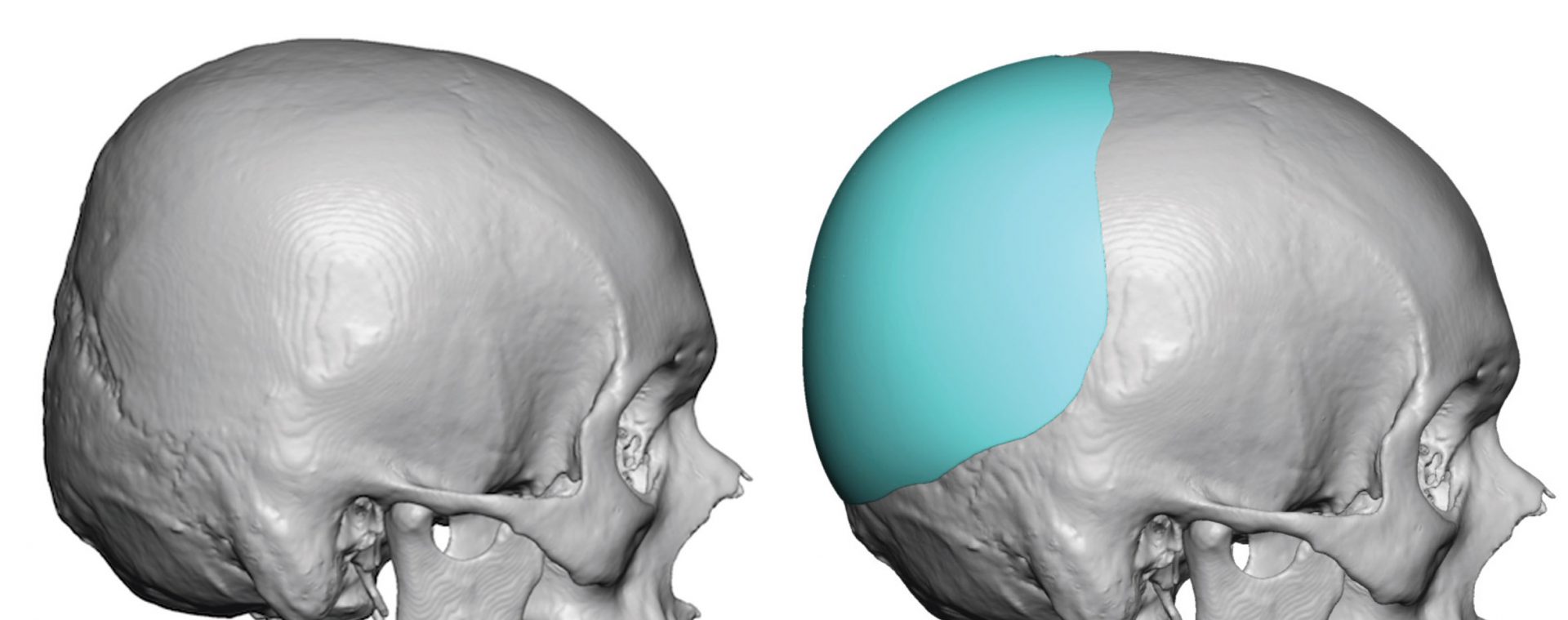
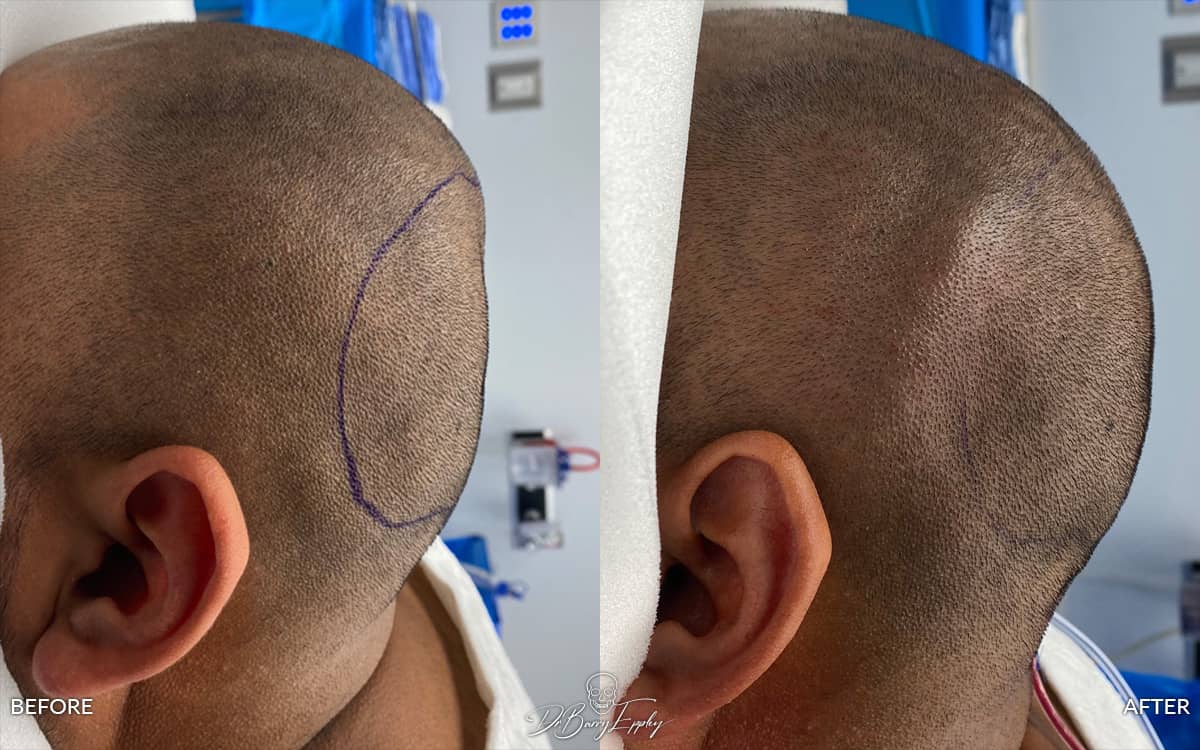
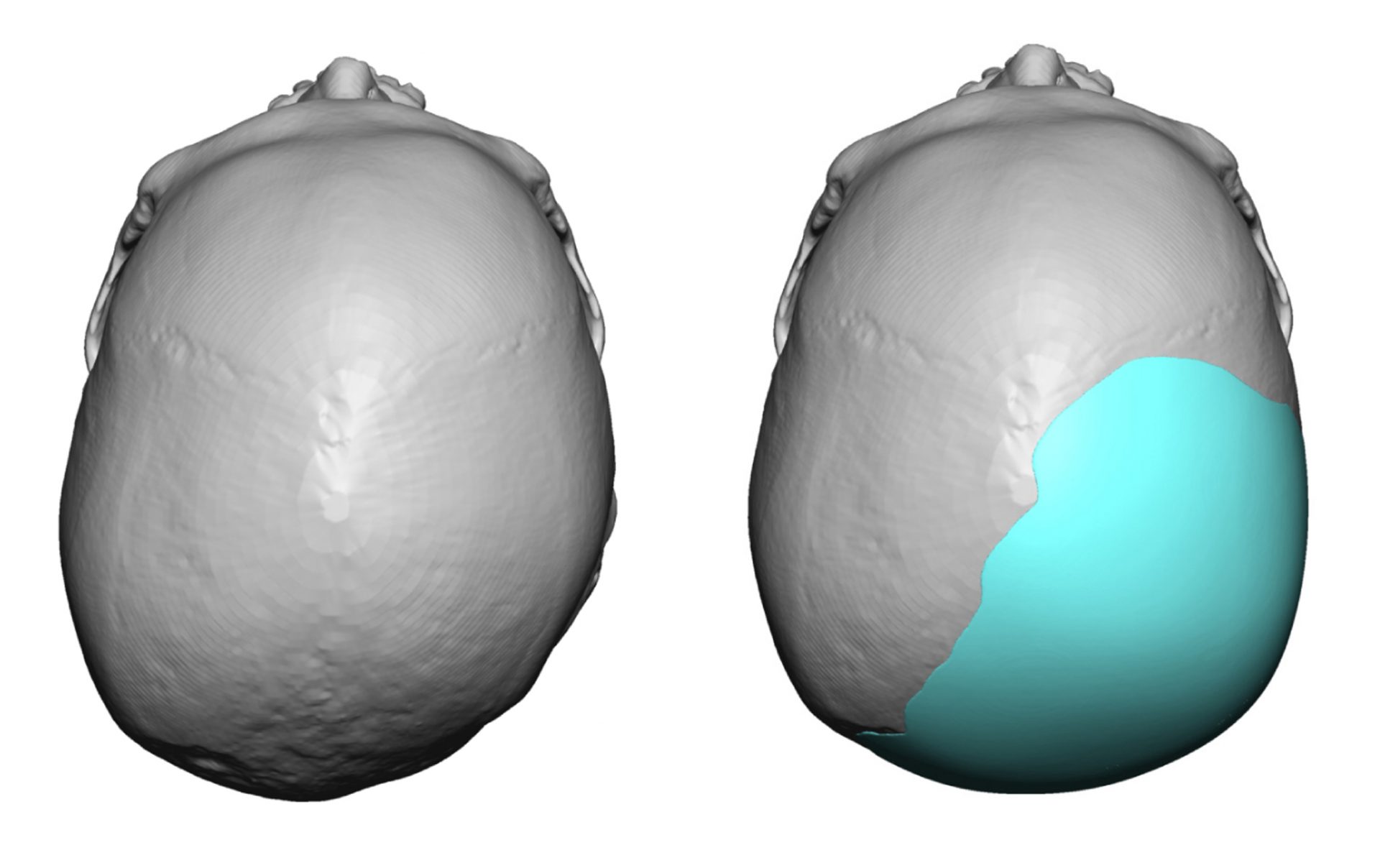
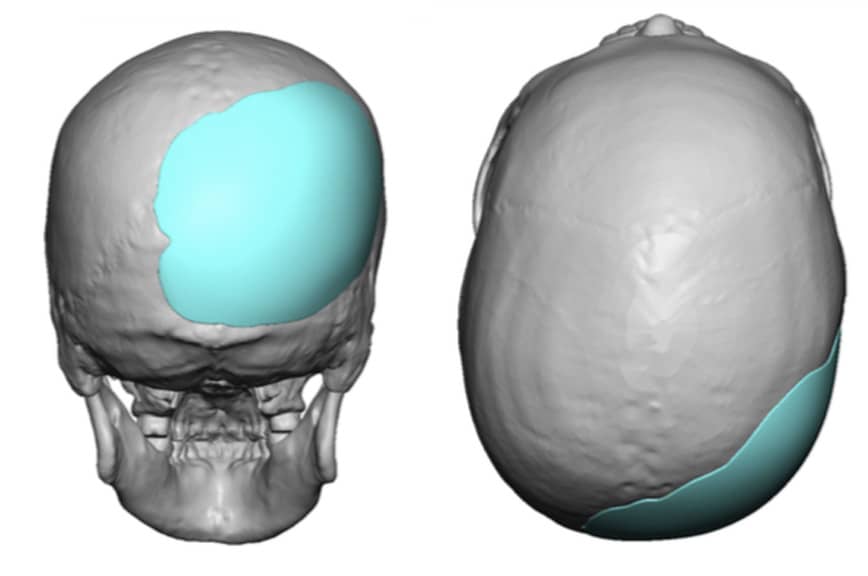
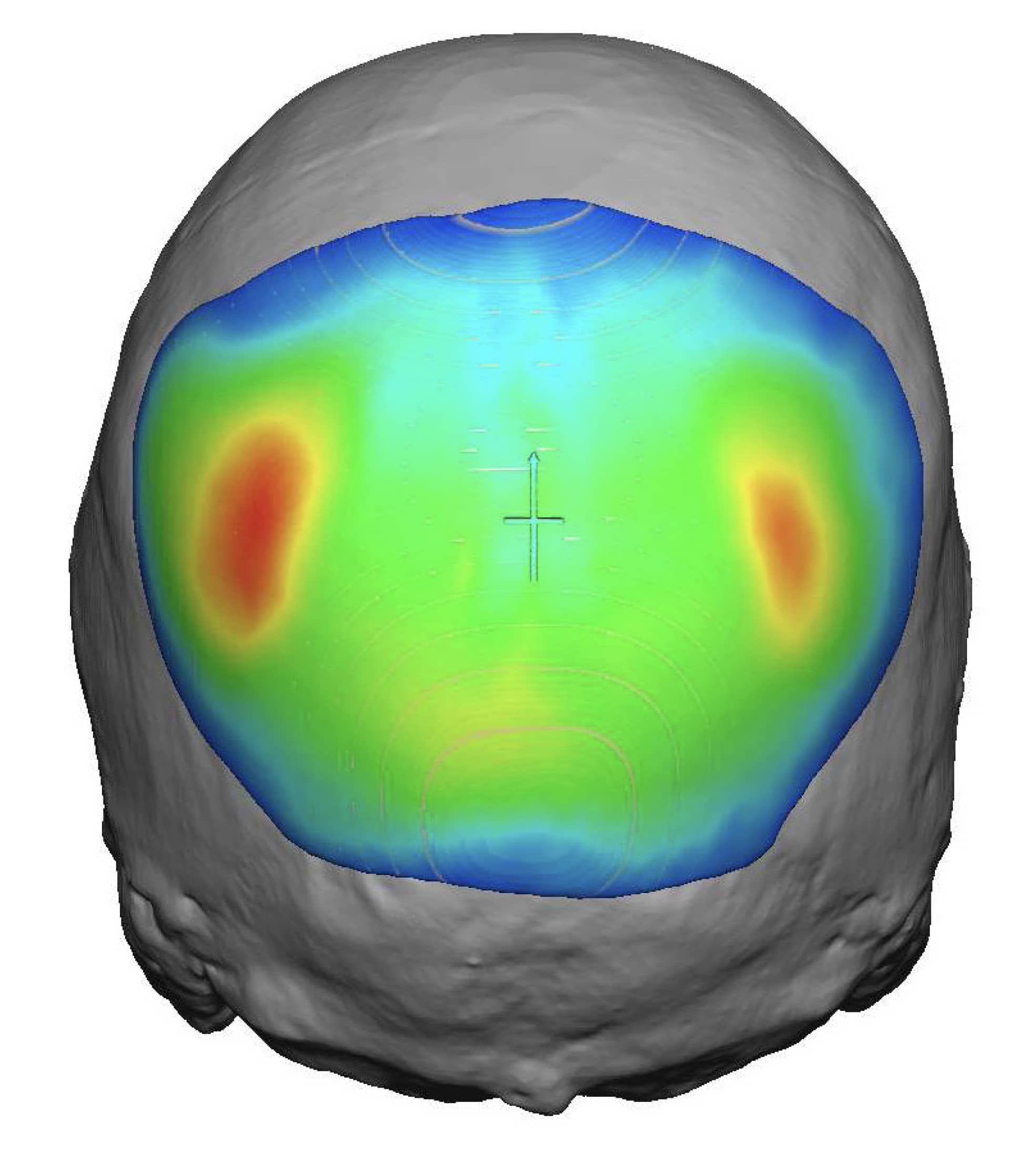
The back of the head can have a wide variety of contour irregularities due to its exposure during development, birthing extraction and after birth head positions. This is most commonly reflected in flatness of one side of the head known as Plagiocephaly. This well known head shape deformity technically involves the entire skull (cranial scoliosis) but often presents as most severe on the back of the head. This is ideally treated by the custom implant process where the design can be made that best matches the opposite more normally projecting side.
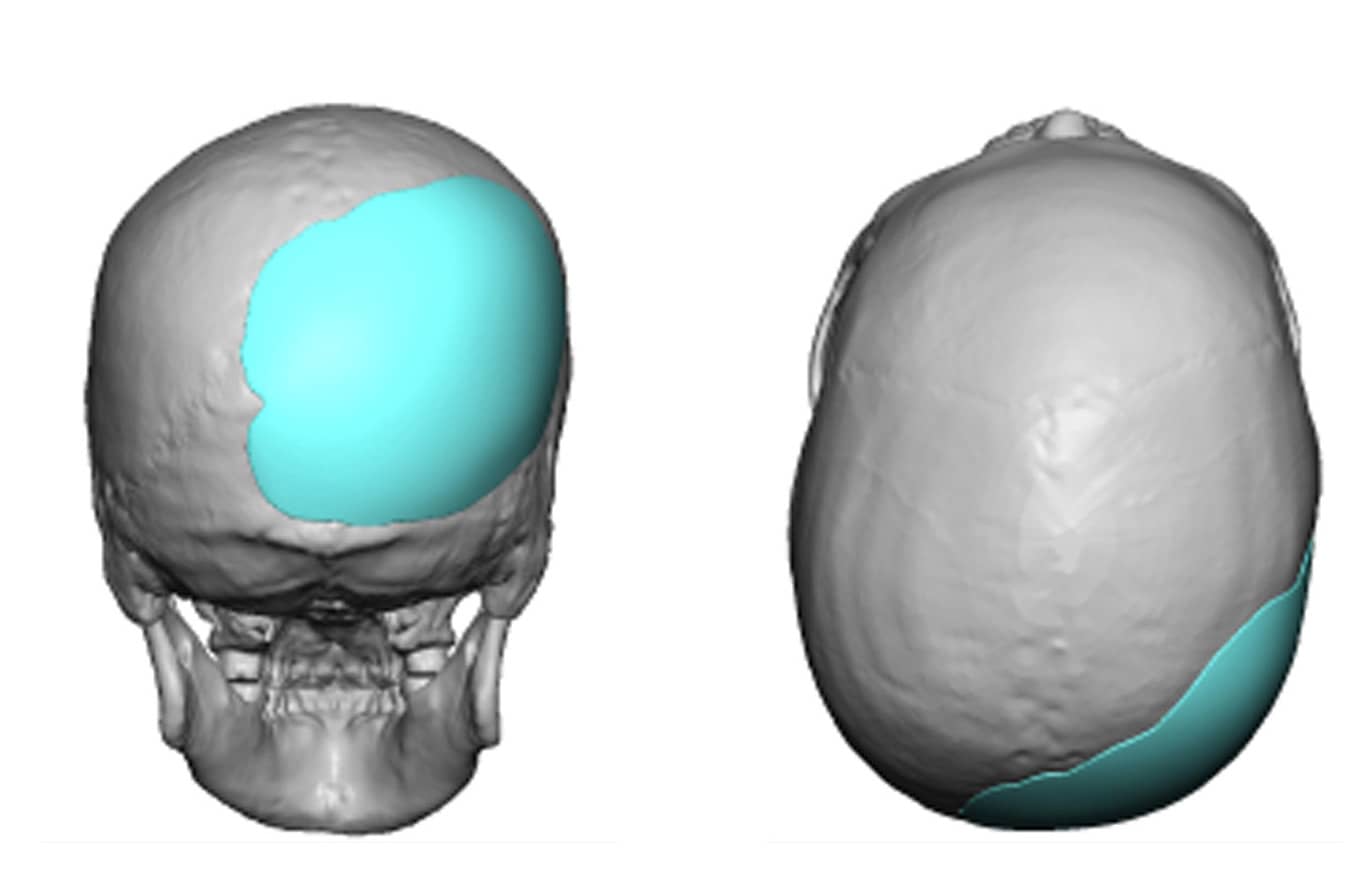




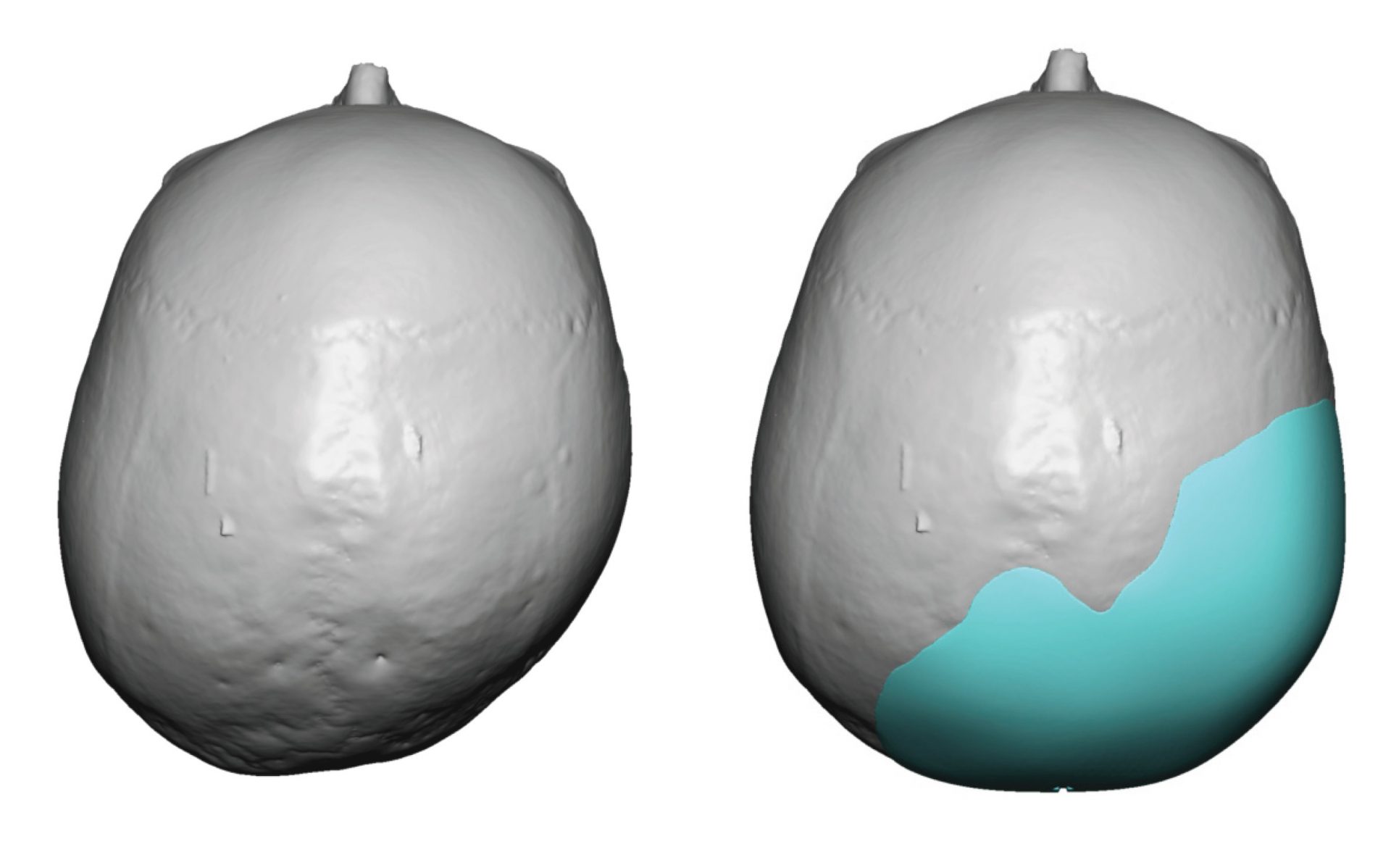
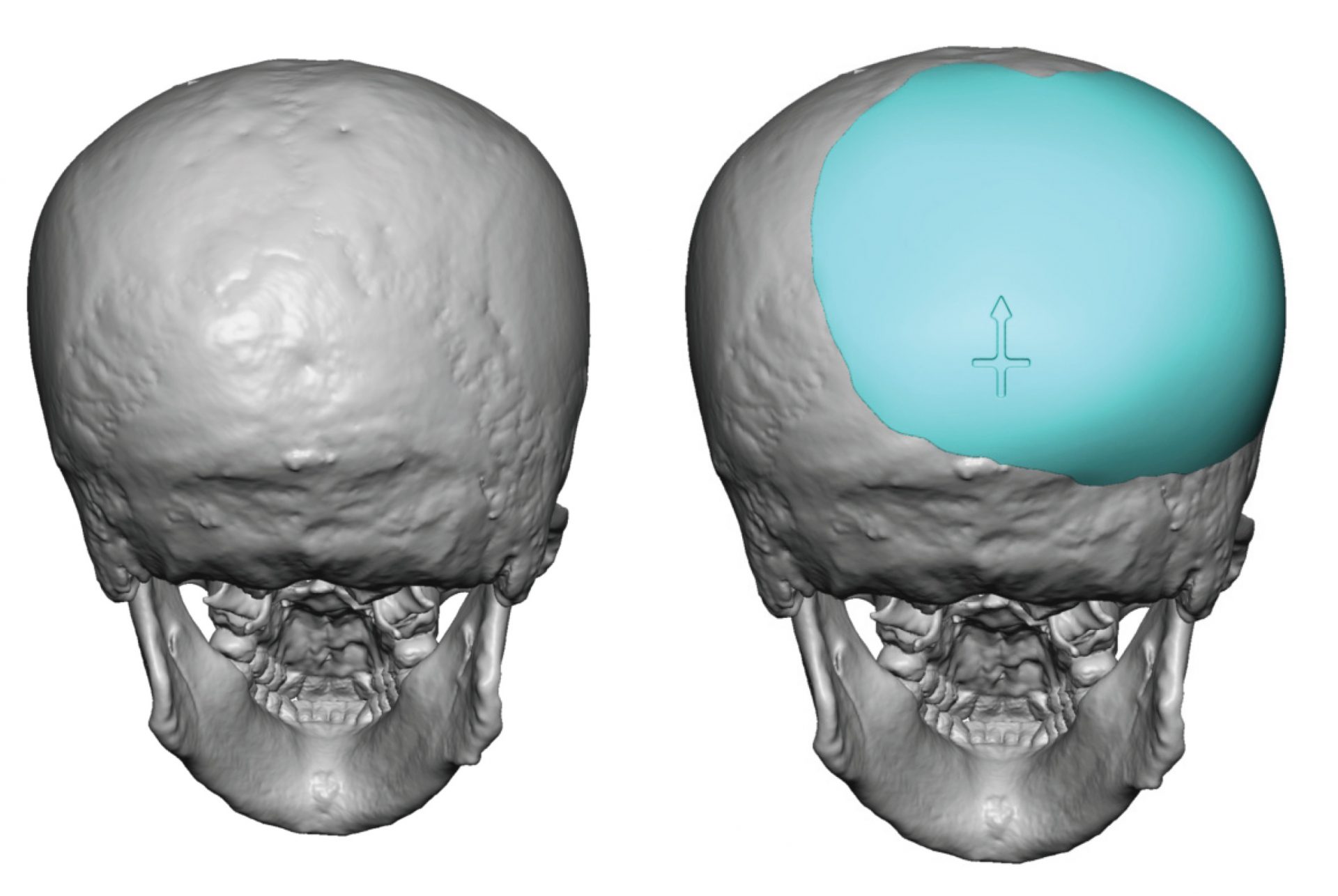
Some plagiocephaly patients may want and/or need not only the flat side corrected but to create an overall increased projection of the back of the head as well.


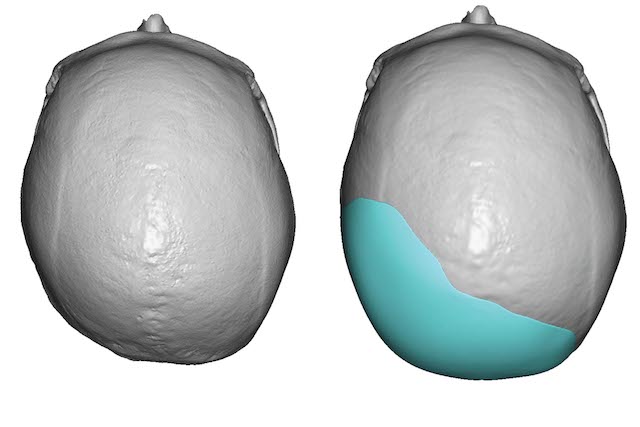
The occipital skull can also have indentations (dents) that also affect both sides whose origins are not as clear as that of plagiocephaly. A custom skull implant is an ideal way to treat such shape issues that allows for the smallest incision possible to place it.

In some back of the head skull deformities the contour deficiencies may extend up onto the top of the skull, most commonly into the parasagittal surfaces. Custom implants can be designed to create a multi-surface skull contour correction.
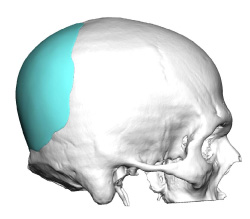
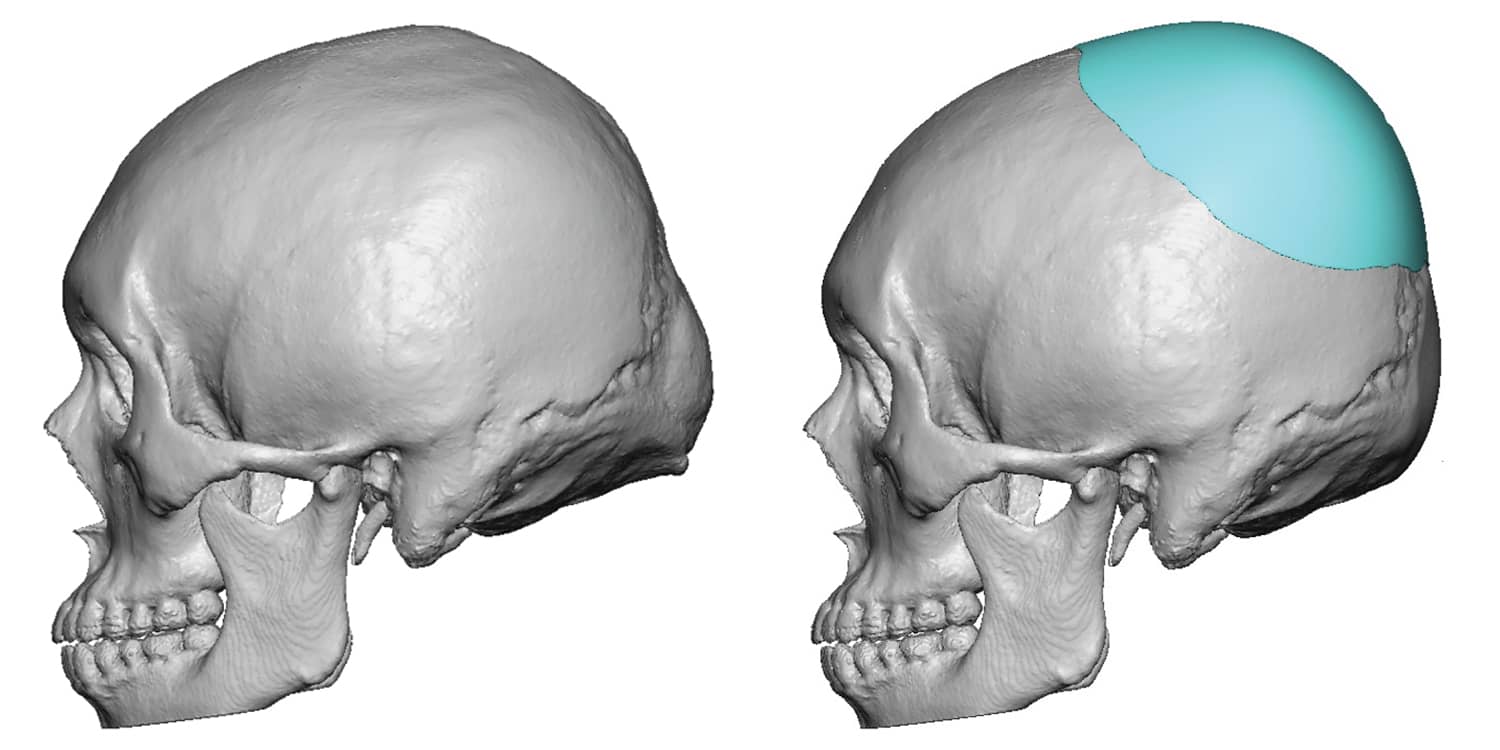
Crown of the Skull Deficiency
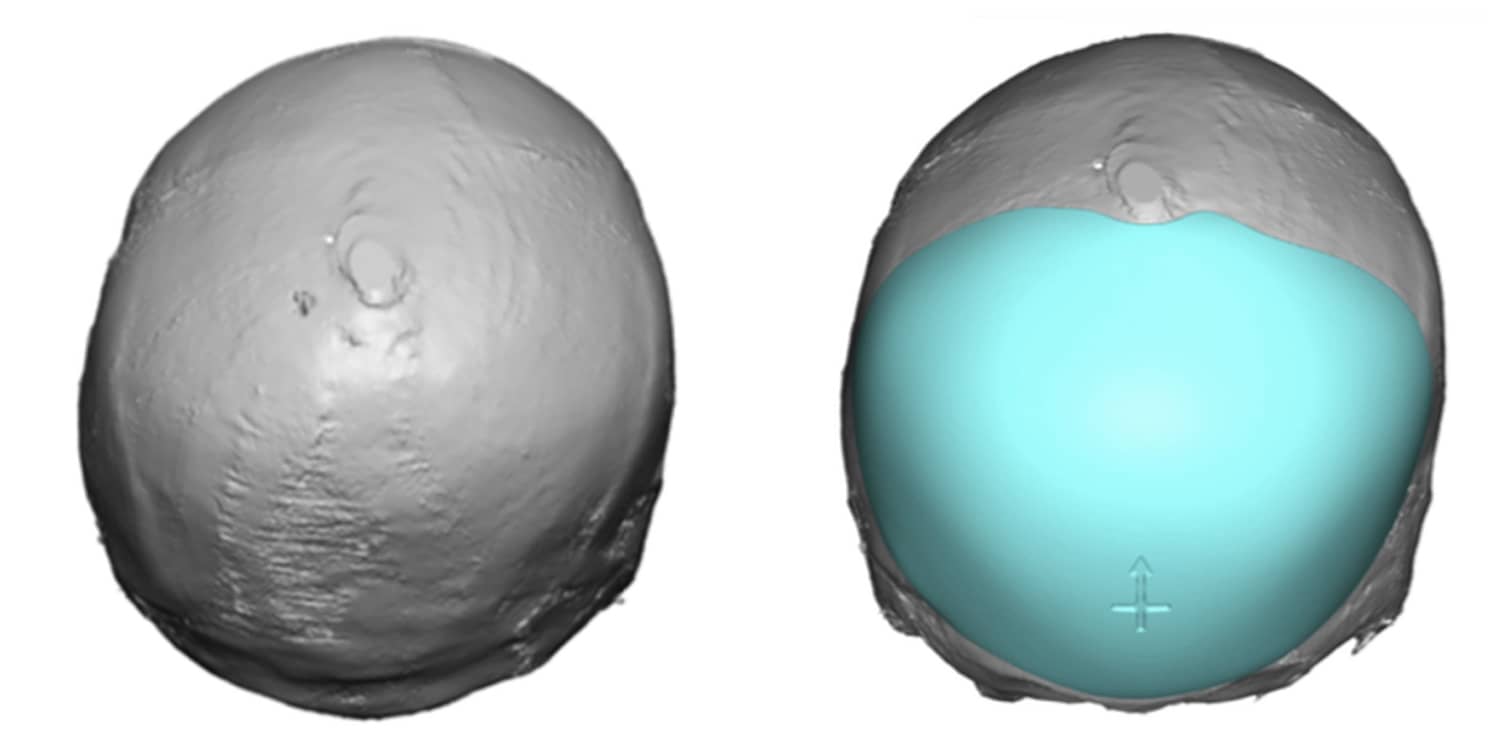
A unique area of occipital deFiciency that is primarily area of concerns for females is the crown area. Technically the crown of the skull is the junction of the back (occipital) and top of the head. That location is more on the occipital area so it falls into the occipital augmentation category. Creating a more prominent crown to the skull is what some women do through hair camouflage techniques to make it look fuller. A custom skull implant is the best method for this type of skull augmentation to achieve a circumferential fullness that its smooth and symmetric. Such an implanted design must cover a much bigger surface area of the skull that one would think. But it must do so to avoid sticking up like an unnatural bump on the back/top of the head.


Back of Head Reduction
Excessive projection or bulging of the back of the head can be partially or completely corrected by a bone burring reduction of the outer cortex of the occipital skull bone. The amount of reduction will be limited to the thickness of the outer cortex which can be determined by measurements on a plain lateral skull x-ray, axial 2D CT images or from 3D CT scan images. Occipital reduction is done through a horizontal scalp incision usually located directly over the most projecting area or lower down at the nuchal ridges at the bottom of the hairline. Some patients prefer a superior approach with an incision at the crown of the head. Whether done from a superior or inferior incision back of head skull reduction can be successfully completed.








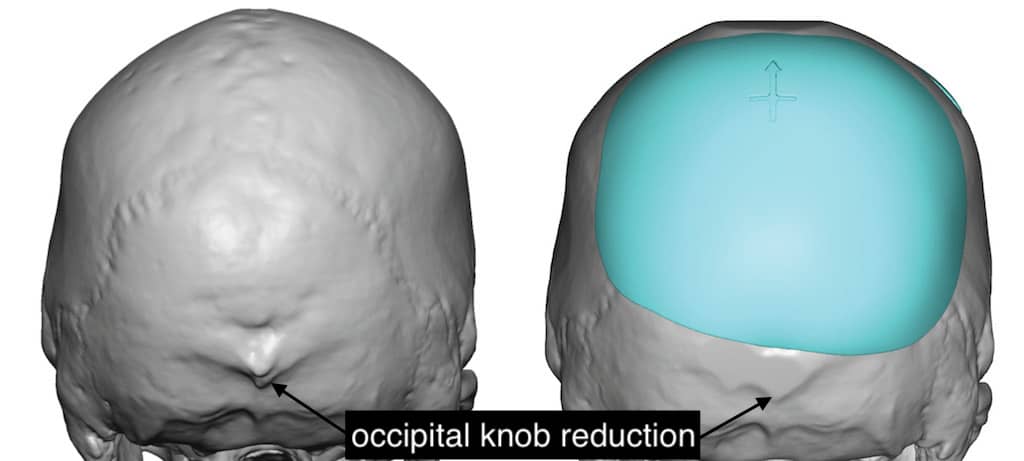
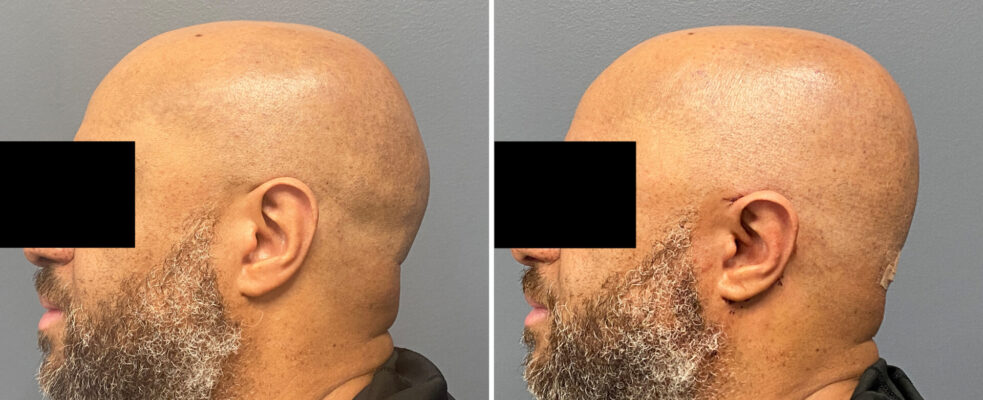
Occipital Knob Reduction
The occipital knob is a central projection of bony overgrowth on the lower end of the occipital bone. It is a very distinct and usually round bone thickness that produces a prominent bump or knob at the midline of the nuchal ridges. In some patients, its size can be quite striking and really sticks out in the male who shaves his head or has very closely cropped hair. It can be completely reduced by a rotary burring of the excess bone through a very small horizontal scalp incision directly over it.






Occipital knob reductions can be combined with custom skull implants in some patients who have a flattening of the back of the head above the knob area. This produces a synergistic effect of creating an improved convex shape of the back of the head.
Occipital Nuchal Ridge Reduction
Nuchal ridges are horizontal bony lines that aesthetically mar an otherwise smooth back of the head contour. The nuchal ridges can be flattened by burring down their prominences to a smoother contour that blends better into the bone around them.


Occipital Bun Reduction
The term ‘Occipital Bun’ can have several different meanings but it always refers to a protrusion on the back of the head. Not to be confused with the occipital knob or nuchal ridge protrusions this specifically refers to an overgrowth of the entire occipital bone. As a result the protrusion stops at the level of the lambdoid sutures which creates a rounded protrusion or bun appearance in side view. This can be reduced through a horizontal incision located at the level of the nuchal ridge in which the outer layer of the skull bone down to the diploid space can be removed by a high speed burring technique. There are limits as to how much bone can be removed but visible improvements are always obtainable…even if they may not always remove as much as the patient would like.

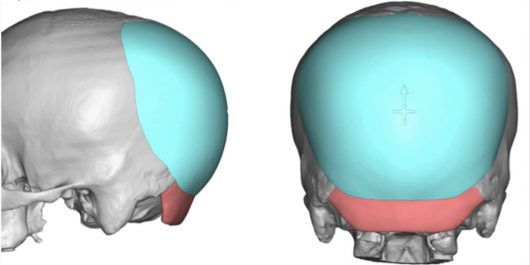
There are some cases of an occipital bun protrusion where there is a flatter area skull area above it. This combination of a lower occipital protrusion combined with an upper parietal bone flattening requires the need for a dual approach to an optimal back of the head reshaping. The occipital bone reduction can be combined with an augmentation above it (custom skull implant) to get the best profile shape to the back of the head.

Locations
Carmel, IN 46032 USA
Contact Us