Aesthetic Skull Surgery for Side of The Head Reshaping (Temporal Augmentation and Temporal Reduction)
On this Page
Temporal Hollowing
The most traditional concept of temporal hollows or concavity is the temporal region between the eye and the temporal hairline. (the anterior temporal region) Situated just above the zygomatic arch, deepening of this temporal region is well known to occur from fat loss due to aging, disease (medical conditions that cause facial lipoatrophy) or simply as part of one’s genetics and natural facial structure. This is historically the part of the side of the head that is believed in plastic surgery to be subject to change.
Aesthetic augmentation of the anterior temporal concavity is most commonly done by injection techniques using various types of injectable synthetic fillers or one’s own processed fat. While these injection methods do have potential effectiveness, the duration of their effect is not guaranteed nor is the consistency of the augmentation. Preformed temporal implants are now available that provide a simple and permanent temporal augmentation effect. These are very soft silicone implants designed to feel like the muscle tissue onto which they are placed. The implants are placed in a subfascial location on top of the muscle through small vertical incisions placed back behind the temporal hairline. The traditional or type 1 standard temporal implant provides augmentation to the deepest part of the temporal hollow down closer to the side of the eye.




For correction of a temporal concavity that extends beyond the lower half of the non-hair bearing temporal region, extended silicone temporal implants can be used to provide an augmentation effect all the way up to the side of the forehead at the anterior temporal line. While this style of temporal implant (Type 2) is longer (vertically higher), it does not require a bigger scalp incision to properly position it into place.


The Narrow Head
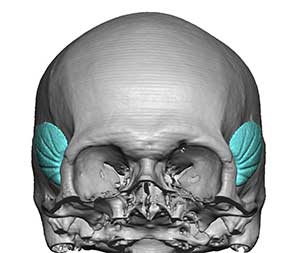
The perception of a head that is too narrow relates to the shape of the side of the head above the ears in many patients so affected.. This is the posterior temporal region and is actually much bigger than the anterior temporal area in terms of surface area. When the sides of the head lack any convexity (vertically flat), they can look too narrow. Just like the anterior temporal region, the posterior temporal area can be augmented as well by placing a silicone implant under the temporal muscle or under its fascia depending upon the size of the implant. Such head widening temporal implants are custom made based on the patient’s aesthetic needs. Because of its surface area coverage the implant does not need to be overly thick to have a significant augmentation effect. The posterior temporal or head widening implant is usually placed through an incision in the crease at the back of the ear for a completely hidden scar.

Extended or Complete Temporal Augmentation
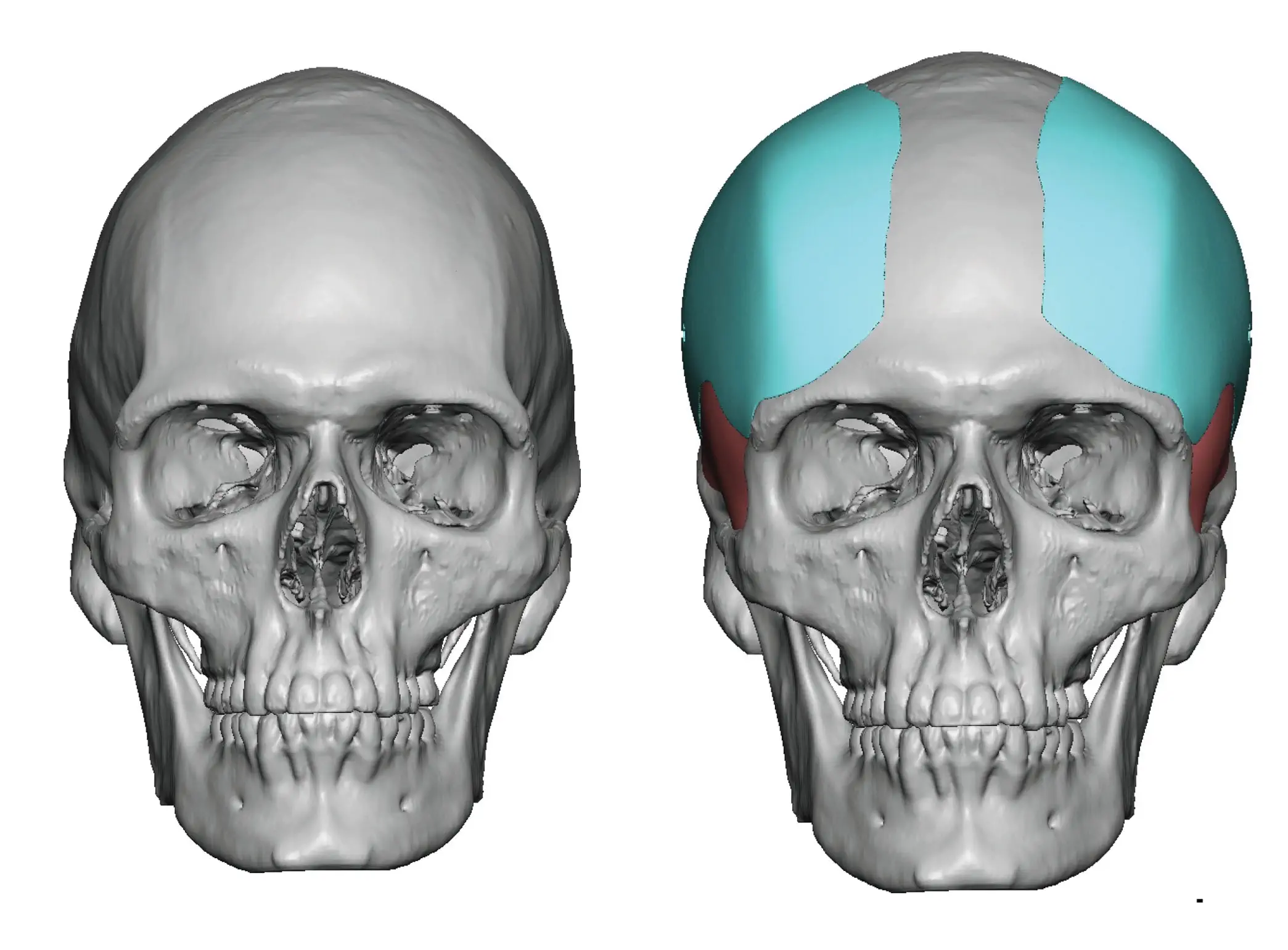
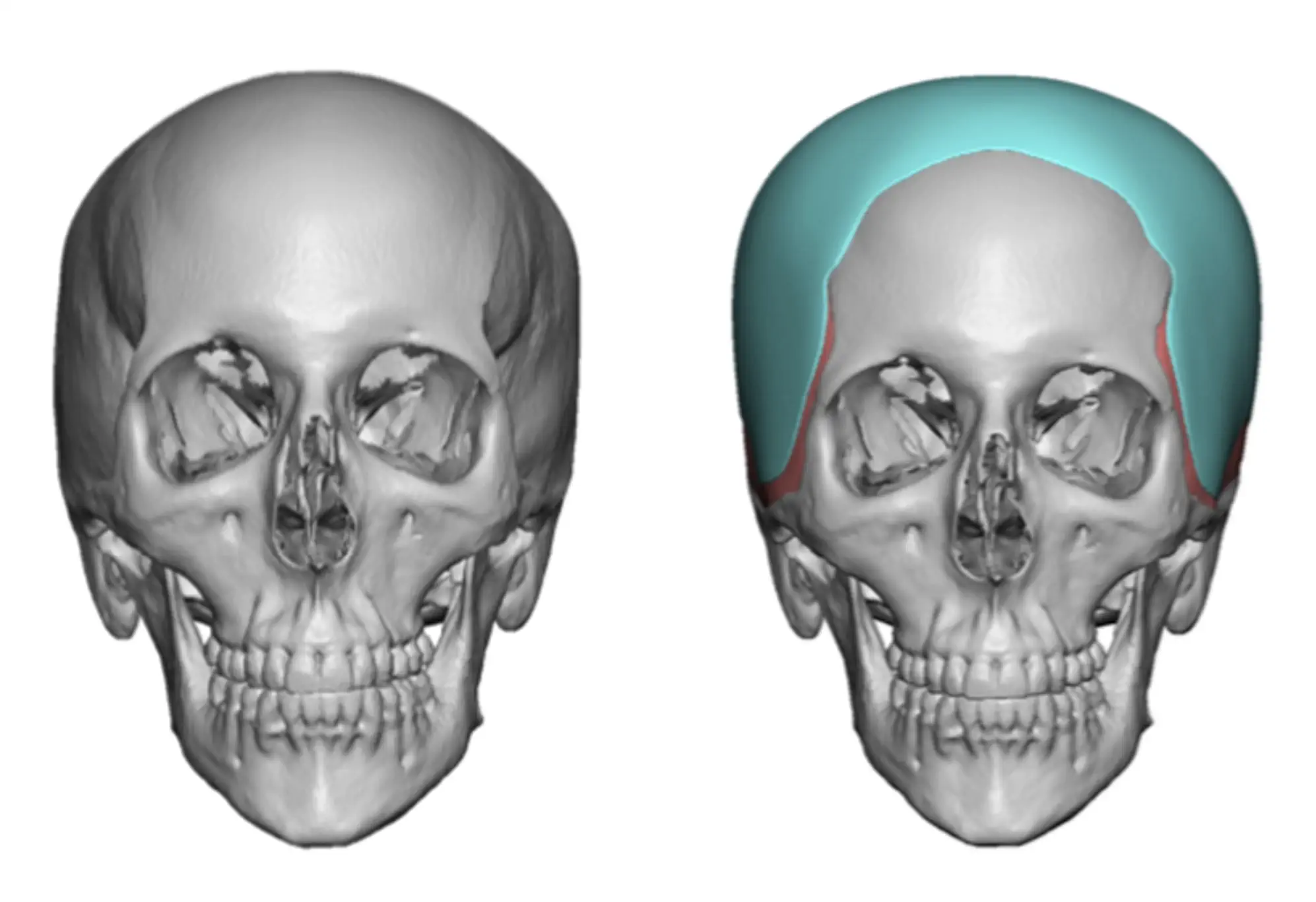
Augmentation of the complete side of the head from the side of the eye back to the front edge of the occipital area (posterior temporal line) can be done by several techniques. One approach is to combine standard style 2 temporal implants with custom posterior temporal implants. This works best when the augmentation does not need to cross the anterior and posterior temporal lines and it is important to keep the implants under the fascia and /or muscle. A single vertical incision in the scalp above the ear or an incision placed behind the ear in the postauricular sulcus can be used to place both types of temporal implants.

The most complete or total temporal augmentation crosses the temporal lines and extends beyond the anterior temporal lines of the forehead and the posterior temporal lines on the back of the head. A one-piece custom wrap around temporal implant is is used to cover the entire side of the head from the forehead to the back of the head onto the occiput-parietal skull area. Placed through an incision behind the ear supplemented with one or two smaller ones in the scalp for endoscopic placement guidance and screw fixation, this large coverage temporal implant provides a definitive correction of the narrow or scaphocehalic head shape.

Narrow temples can also be associated with an overall smaller head as well, crossing over the temporal lines and including the whole top of the head. A custom skull implant can be designed to improve the contour across the top of the head as well as that of the temples. Such an implant design is placed through a scalp incision across the top of the head.
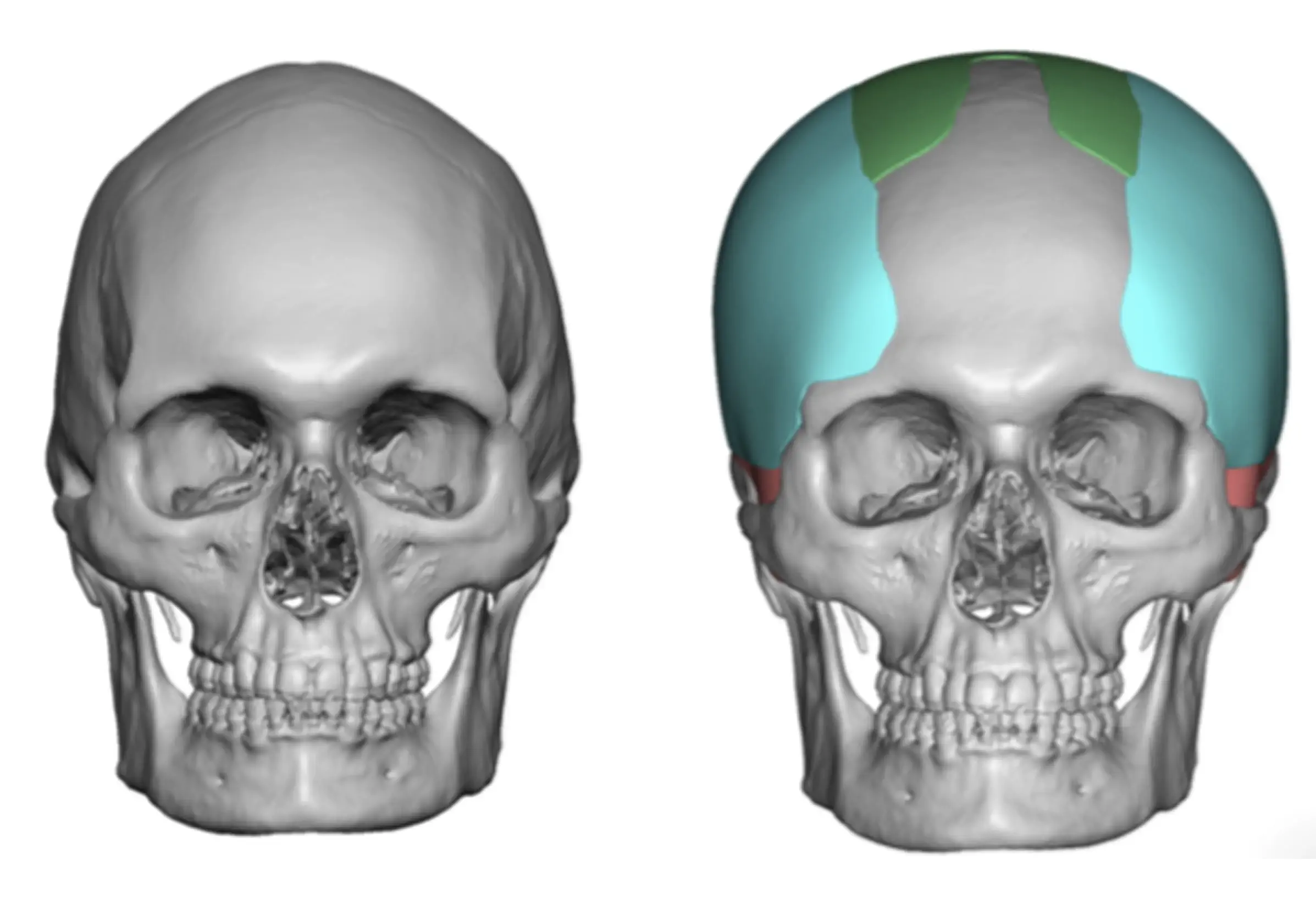
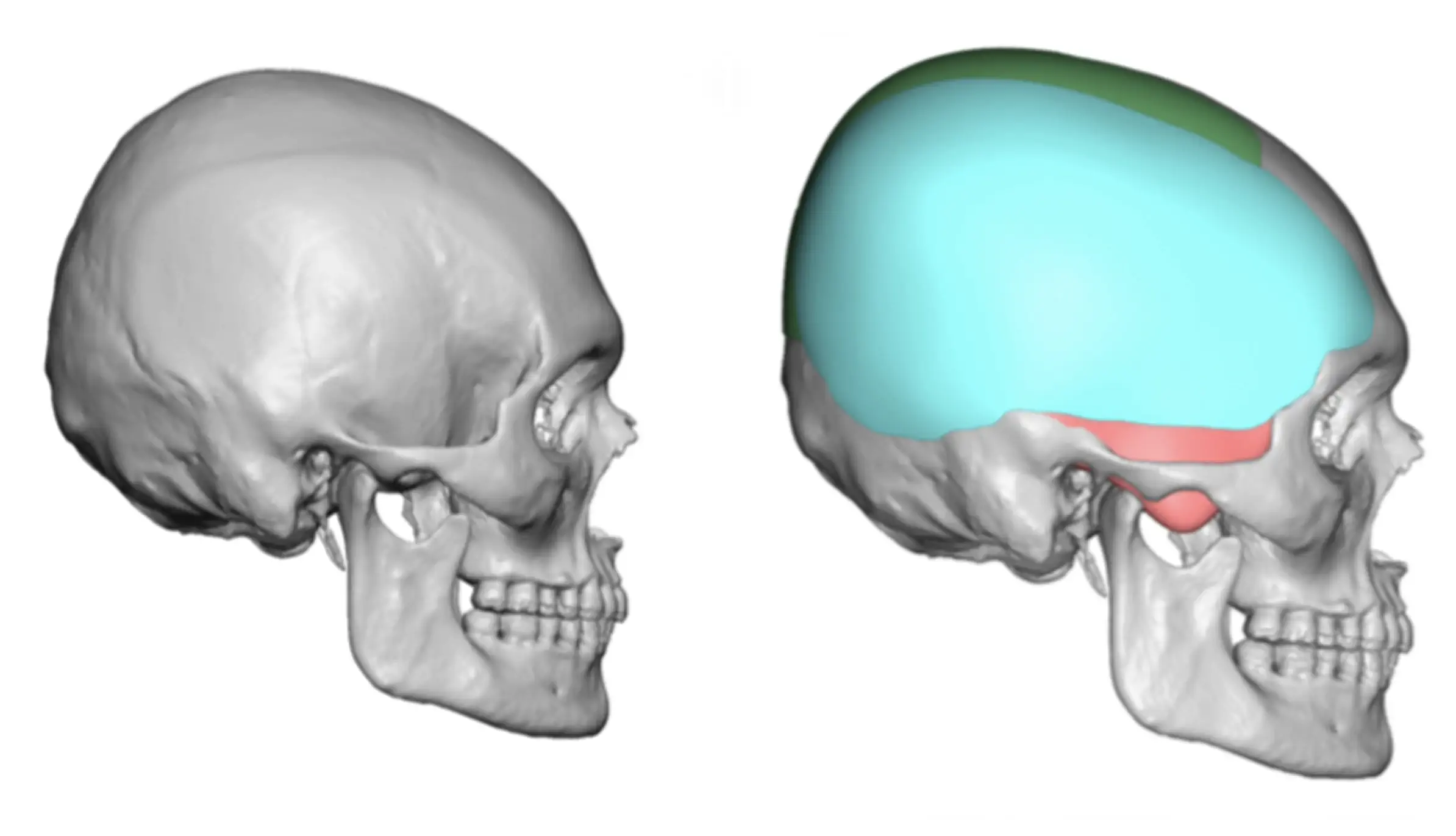


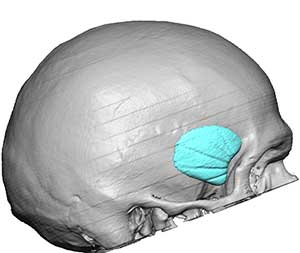
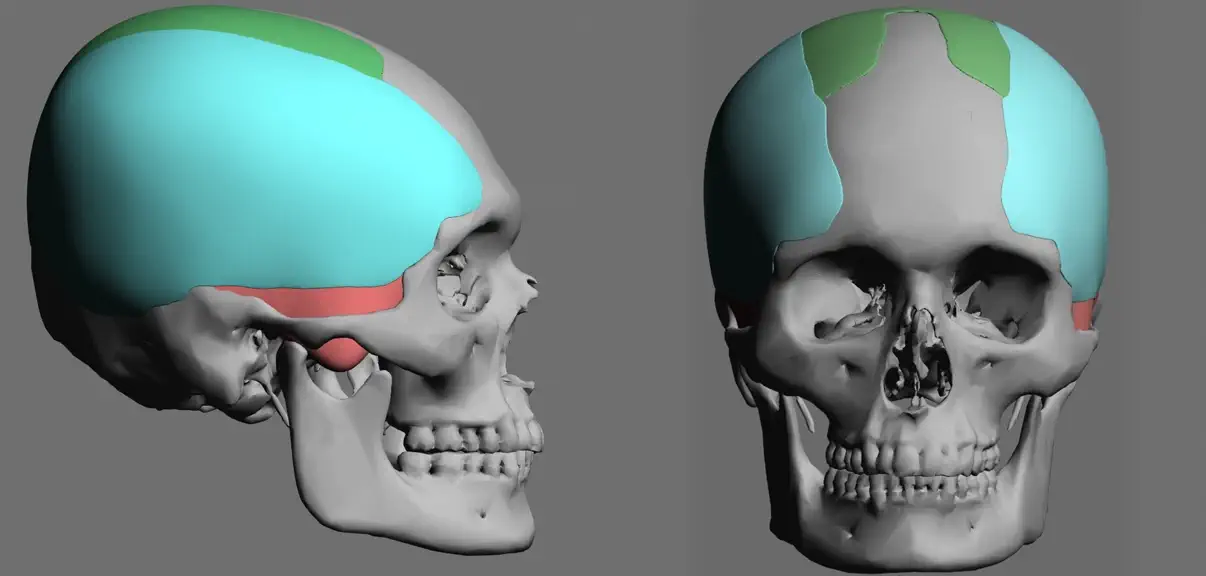
A temporal deficiency can also be part of a very common congenital skull shape deformity, plagiocephaly. The side of the flatter back of the head can extend forward along the side of the head into the posterior temporal region. A custom skull implant can be designed that augments both the flat back of the head as well as the posterior temporal region. In this case the pocket location is a dual subperiosteal and on top of the deep temporal fascia. When done as part of an overall skull reshaping approach, it is used in some cases as a secondary implant after other skull implants that have been previously placed. (in green color) Like most custom temporal implants they are placed primarily from a postauricular crease incision. (behind the ear)

Wide Head Reduction
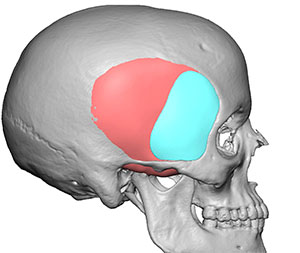
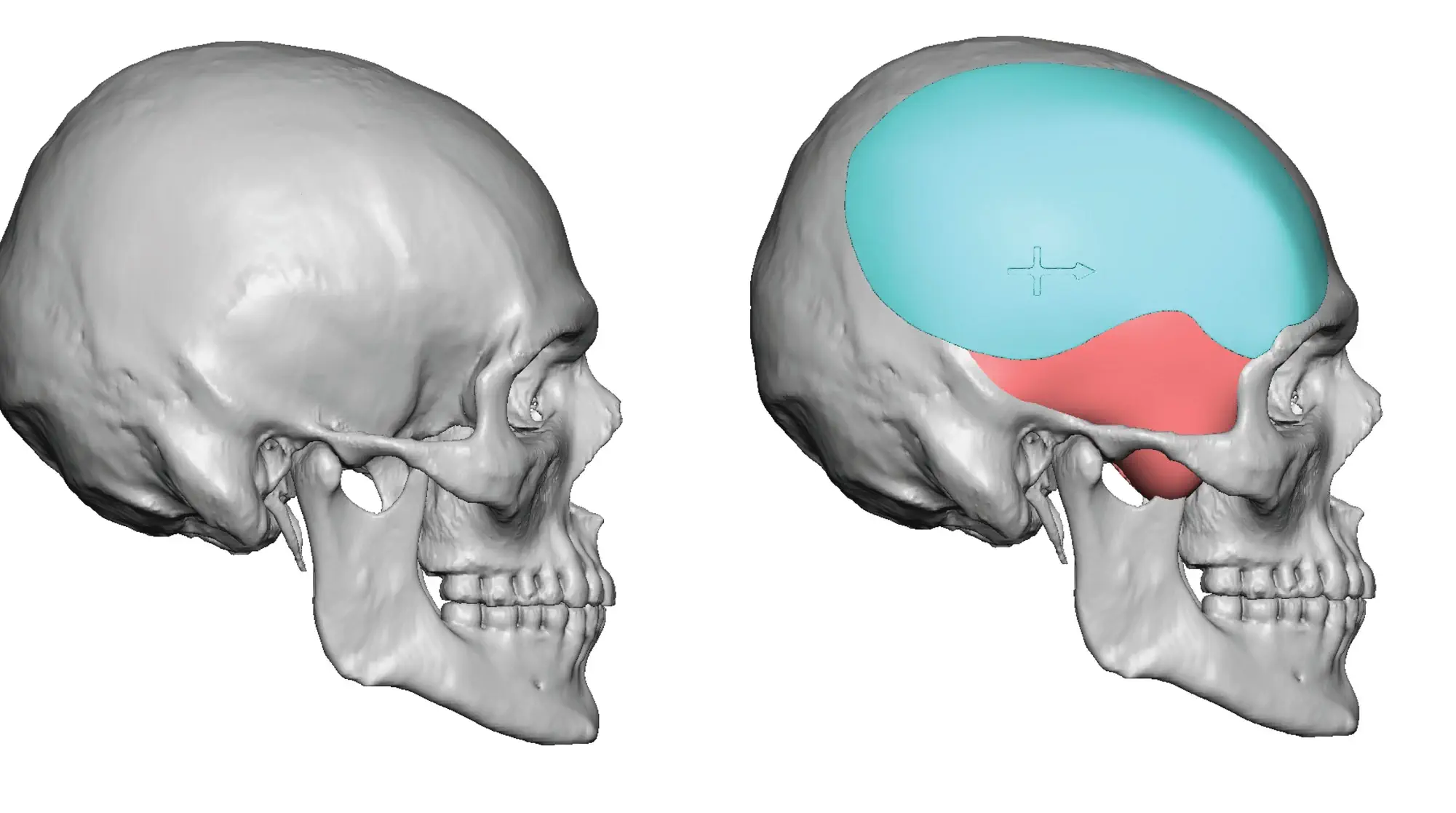
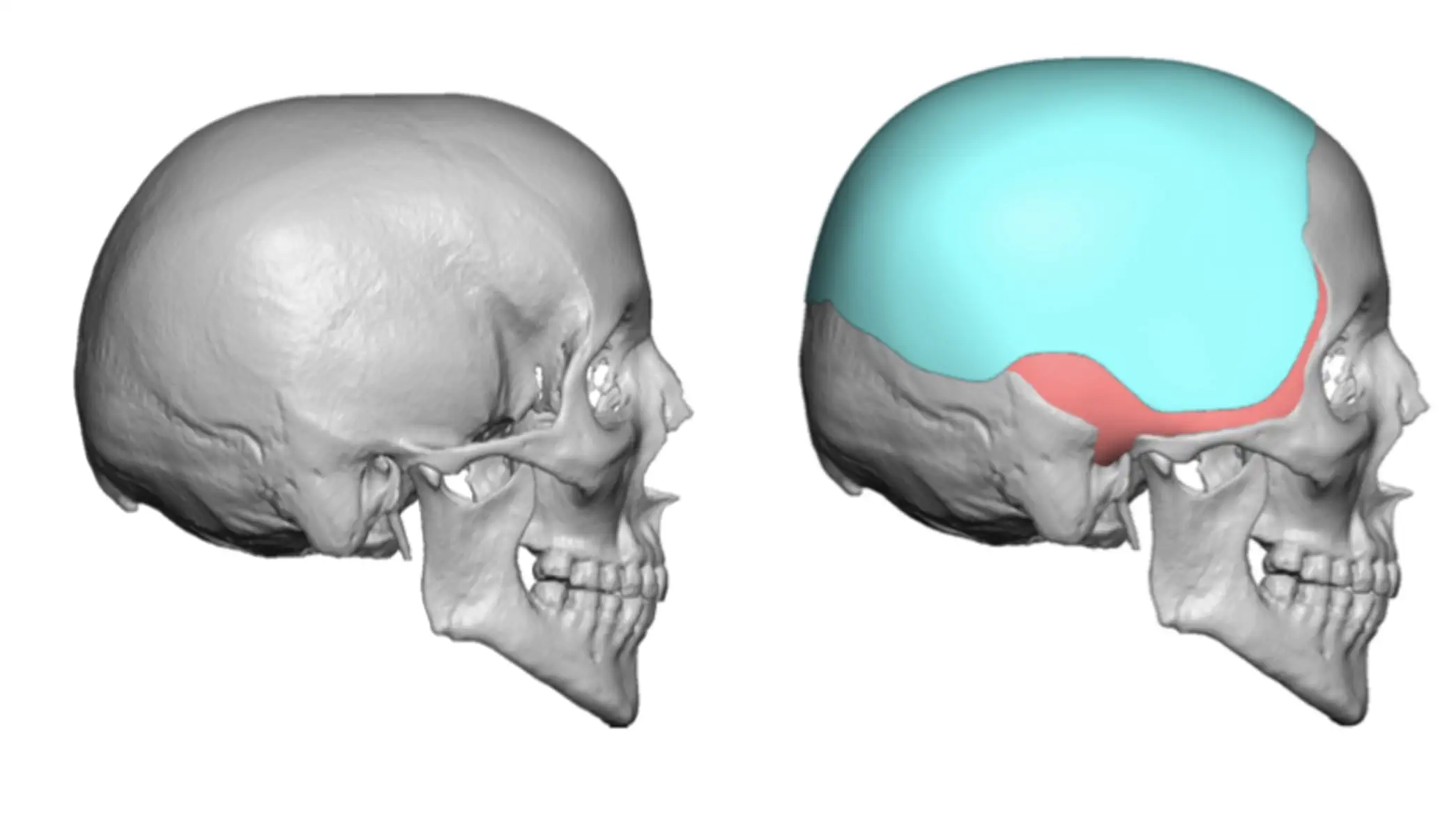
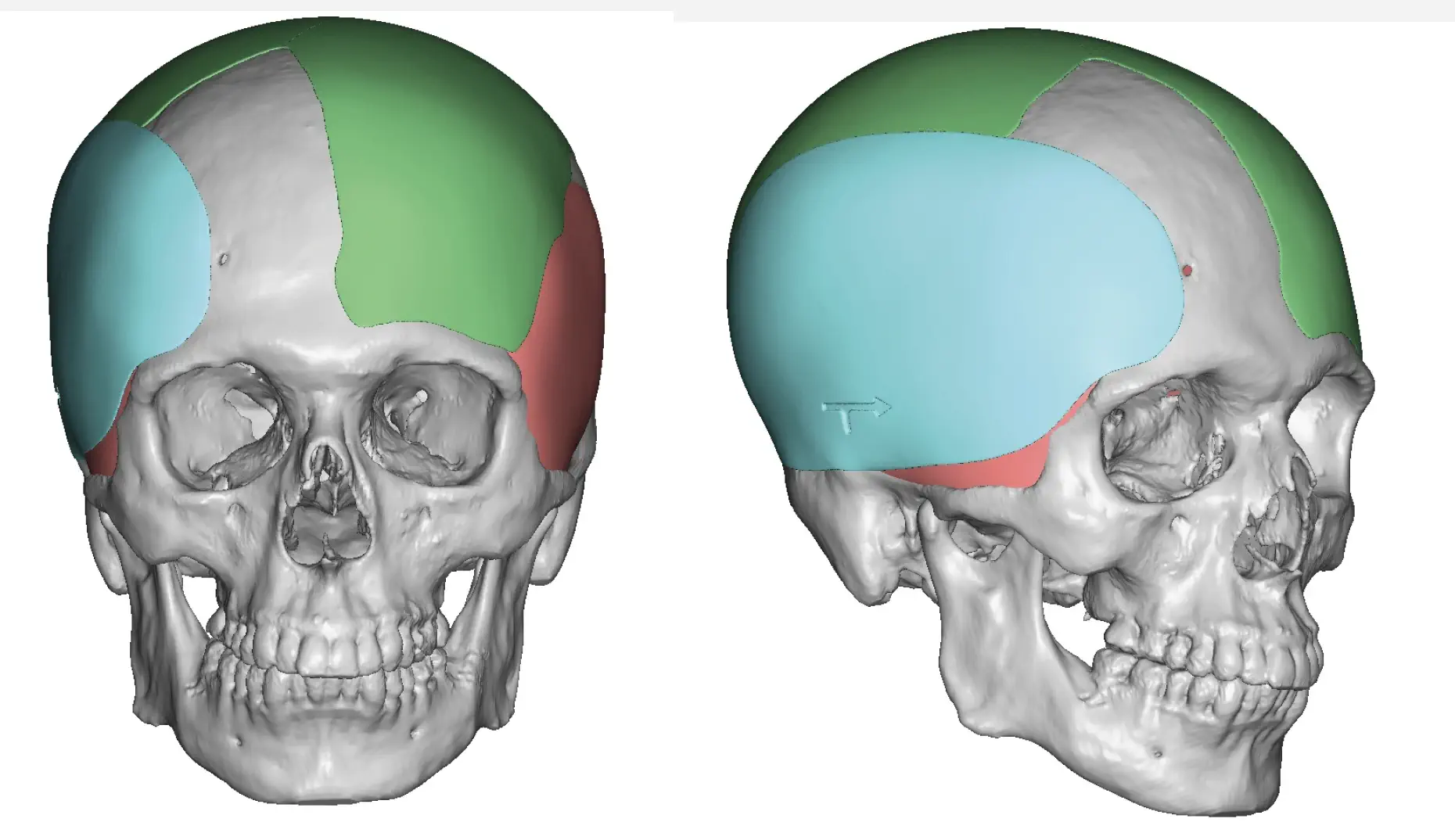
Just like a narrow side of the head can be augmented, an overly convex or too wide side of the head can be reduced. The key anatomic understanding of a wide side of the head is to determine is this in the anterior (blue outline) or posterior temporal regions (red outline) or both. That distinction is important as the potential treatments vary amongst these two areas. In the anterior temporal region reduction is most reliably done using Botox injections. Surgical muscle excision can not be done in this temporal area. There are some techniques for anterior temporal muscle release which can have some effectiveness, but neuromuscular blocking agents should be the initial approach in many cases. While usually not permanent and needing to be repeated, Botox has a well known history of clinical effectiveness at reducing the size of masticatory muscles. It is also a simple and safe technique that has no known side effects.
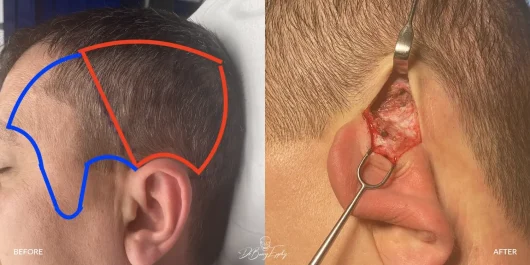
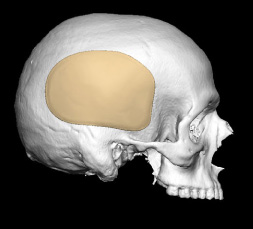
While Botox injections can also be done in the larger posterior temporal muscle area as well, surgical removal of the posterior temporal area provides an immediate and permanent effect. While many think the excessive convexity at the side of the head is due to the thickness of the temporal bone above the ears, the posterior temporal muscle is often as thick as the bone if not thicker. By tissue ratios, it makes up a greater portion of the posterior temporal convexity often being as thick as 7mm to 9mms between the overlying fascia and the underlying bone. Removal of the posterior temporal muscle can be done through a small incision behind the ear with an immediate and dramatic flattening of the temporal convexity and width of the side of the head. Removal of the posterior temporal muscle causes no problems with opening and closing the lower jaw due to the size of the remaining anterior belly of the temporal muscle.










Prominent Temporal Arteries
One very unique type of aesthetic temporal deformity is not associated with the muscle or bone. Rather it is an anomaly of the blood vessels specifically that of prominent temporal arteries. These are characterized by having a visible tortuous or serpiginous course across the temples into the forehead. They are caused by the enlargement of the superficial temporal artery. (STA) The anterior branch of the superficial temporal artery leaves the temporal hairline and crosses into exposed temporal skin on its way into the forehead. In some people the size of the anterior temporal branch artery becomes large and visible. When exercising, exposed to heat, bending over or any activity that increases the heart rate, the course of the artery bulges and becomes glaringly conspicuous. It may occur on just one side or be asymmetrically prominent.

Creating a long and tortuous bulging vessel, some patients may seek a reduction in its prominence. Temporal artery ligation can be safely done through very small incisions (5mms or less) to decrease its forward blood flow and either reduce or eliminate the prominence of the vessel. At least two points of ligation are always needed (sometimes 3 or 4) to prevent backflow and/or catch unseen branches that may be feeding into it. This is usually done as an outpatient procedure under local anesthesia. It does not have any adverse side effects on the scalp such as hair loss or scalp skin issues.



Locations
Carmel, IN 46032 USA
Contact Us
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.